Download
1 / 22
570 likes | 2.01k Views
LISFRANC INJURIES. James M. Steinberg, D.O. Garden City Hospital. Historical Perspective. Tarsometatarsal joints Fracture-Dislocations Named for Napoleon’s surgeon Dr. Lisfranc Injury was common in cavalry troops Due to design of the stirrup Severe vascular complications

E N D
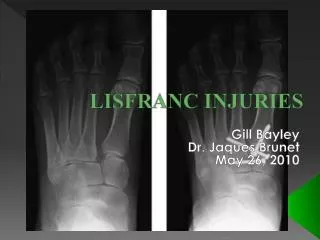
LISFRANC INJURIES James M. Steinberg, D.O. Garden City Hospital
Historical Perspective • Tarsometatarsal joints • Fracture-Dislocations • Named for Napoleon’s surgeon • Dr. Lisfranc • Injury was common in cavalry troops • Due to design of the stirrup • Severe vascular complications • Amputation was performed
Etiology • Injuries to tarsometatarsal joints of the midfoot constitute ~0.2% of all skeletal fxs • As many as 20% of these injuries have been reported to have been missed initially • Myerson et al. reported a 4% incidence per year in collegiate football players • Five tarsometatarsal joints are very stable & immobile • Usually sustain acute injuries from high-energy forces
Mechanism of Injury • MVA • Industrial accidents • Sports injuries • Football: direct axial loading onto the heel of a foot fixed in equinus • Equestrian: rider gets foot caught in stirrups while falling from horse • Wind surfing: straps to allow for pivoting cross midfoot, similar to stirrups • Running/Walking: foot caught in hole or mis-step off a curb, excessive ankle equinus
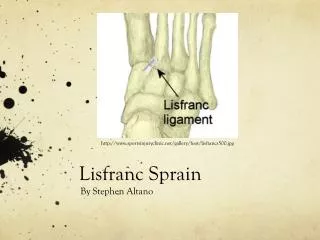
Anatomy • Lisfranc’s joint: • Key to the transverse arch of the foot • Lisfranc’s ligament attaches the medial cuneiform to the base of the 2nd metatarsal • Continued ligamentous support linking the bases of the 2nd-5th metatarsals • No ligamentous connection between the 1st and 2nd metatarsals • Allows for frequently seen divergent injury • Dorsalis pedis dives between bases of 1st & 2nd
Anatomy • 2nd MT is recessed between the medial and lateral cuneiforms: • “Keystone” mortise that greatly adds stability in transverse plane
Anatomy • Cuneiform, tarsal bones, and medial 3 MT bases: • Have a trapezoidal configuration that is wider on the dorsal aspect • Effect of a Roman arch; resisting collapse
Physical Exam • Diagnosis requires high index of suspicion • Midfoot swelling & tenderness • Often in patients with polytrauma • Vascular status • Assess soft tissues • Open fx • Degloving injuries • Monitor for compartment syndrome
Radiographic Evaluation • AP, lateral, and oblique films • Medial border of the 2nd MT should line up with the medial border of the middle cuneiform on the AP • Medial border of the 4th MT should line up with the medial border of the cuboid on the oblique • No displacement on the lateral, “piano key” • Flake fxs of the base of the 2nd, no matter how innocent, are pathonemonic for Lisfranc disruption
Radiographic Evaluation • Stress views in less obvious but suspected cases • Performed under anesthesia • Forefoot is held in abduction on AP & in plantar flexion on the lateral • CT scans • Useful in evaluating comminution of tarsometatarsal joints and subtle malalignments • MRI • Can identify ligamentous damage • Does NOT offer any significant advantage to determine treatment
Classification • Quenu & Kuss • Homolateral: all five metatarsals displaced in same direction • Isolated: one or two metatarsals displaced in same direction • Divergent: metatarsals displaced in both the sagittal and coronal planes
Classification • Myerson • Total incongruity: lateral & dorsoplantar • Partial incongruity: medial & lateral • Divergent: partial and total
Treatment • Operative treatment is indicated for displacement > 2mm of the TMT joint • Some argue for ORIF regardless of displacement • Key to successful outcome is anatomic alignment • ORIF can be attempted as late as 8 weeks after injury for pts < 160 lbs; >160lbs arthrodesis of medial three joints • < 2mm of displacement: • NWB SLC for 6 weeks • WB SLC for an additional 4 to 6 weeks • Follow closely with repeat radiographs to ensure no displacement has occurred
Treatment • Reduction is easiest if performed within 4 –6 hours • Restoration of circulation is critical for soft tissue healing • Compartment syndrome: • Four fascial compartments • Long medial incision to decompress abductor hallucis & deep compartments • Two dorsal incisions betw 2nd & 3rd and betw 4th & 5th to decompress dorsal intrinsic compartments • Extensive vascular compromise • Midfoot level amputation
Closed Reduction • Spinal or general anesthesia • Modified finger traps to great toe and one or two adjacent toes • Longitudinal traction with 5 to 10 lbs • Manipulate foot within 5 minute period in either inversion or eversion • Rarely palpable or audible reduction • Verify reduction on fluoroscopy • Maintain reduction with Steinmann pins/cannulated screws • Final routine radiographs PRIOR to leaving OR
ORIF • Dorsal incision lateral to EHL in the interval between the 1st & 2nd MT • Isolate dorsalis pedis & deep peroneal nerve • Inspect Lisfranc ligament • Reduce cuneiforms if needed • Steinmann pin followed by cannulated screw • Guide wire/drill medial cuneiform to base 2nd MT • Continue fixation as needed to restore anatomic alignment • Multiple constructs • 1st MT to medial cuneiform • Cuboid to base of 5th MT
Post Operative Care • Bulky dressing with posterior splint postoperatively • NWB SLC at 7-10 days postop • PWB at 6-8 weeks • Laterally placed steinmann pins removed at 8 weeks • Medial screws removed at 4 months
Conclusions • Commonly missed injury • Lisfranc joint disruption should be suspected with flake fxs at base of 2nd MT • Anatomic reduction is essential • Nearly all require fixation • ORIF can be carried out with pins, screws or both • Terrible injuries, especially if missed • Debilitating foot pain