Download
1 / 68
740 likes | 1.04k Views
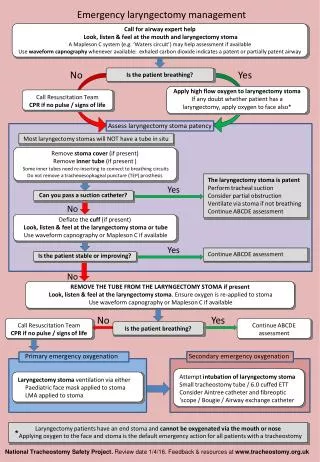
Voice Rehabilitation following Laryngectomy. Balasubramanian Thiagarajan. Introduction. Total Laryngectomy is still the preferred management modality in advanced laryngeal malignancies

E N D
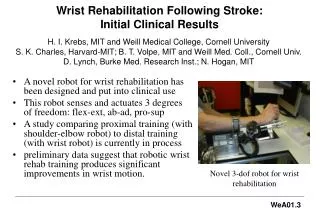
Voice Rehabilitation following Laryngectomy Balasubramanian Thiagarajan
Introduction • Total Laryngectomy is still the preferred management modality in advanced laryngeal malignancies • Advances in medical oncology and radiation oncology combined with traditional surgical methods has increased longevity of these patients • TEP (Tracheo-oesophageal puncture) is considered gold standard among various voice rehabilitation procedures • A good percentage of patients undergoing total Laryngectomy regain esophageal voice • The current 5 yr. survival rate of patients following total Laryngectomy is about 80% An initiative of drtbalu's otolaryngology online
Functional alterations following total Laryngectomy • Loss of smell • Changes in normal swallowing mechanism • Changes in the pattern of respiration • Most importantly Loss of speech. The importance of this function is not realized till it is lost An initiative of drtbalu's otolaryngology online
Components of phonation An initiative of drtbalu's otolaryngology online
Requirements for normal phonation • Active respiratory support • Adequate glottic closure • Normal mucosal covering of vocal cord • Adequate vocal cord length and tension control An initiative of drtbalu's otolaryngology online
Glottic cycle • One opening and one closing incident of glottis is known as glottic cycle • The frequency of glottic cycle is determined by subglottic air pressure • This frequency is unique for each individual An initiative of drtbalu's otolaryngology online
Vocal fold vibratory phases • During phonation two types of vibratory phases occur (Open and closed phases) • In open phase glottis is at least partially open • Open phase can be divided into opening and closing phases • In opening phase the vocal cords move away from one another • In closing phase the vocal folds move closer to each other in unison • Closed phase indicate complete closure of glottic chink An initiative of drtbalu's otolaryngology online
Vocal folds vibratory patterns • Falsetto • Modal voice • Glottal fry An initiative of drtbalu's otolaryngology online
Falsetto vibration • Vocal cord closure is not complete • There is minimal air leak between the cords • Only upper edge of vocal fold vibrates • Also known as light voice An initiative of drtbalu's otolaryngology online
Modal voice • This is the basic frequency at which a pt. phonates • Complete glottal closure occurs during this phase • Vocal fold mucosa vibrates independently of the underlying vocalis muscle • Modal frequency in adult males is around 120 Hz • Modal frequency in adult females is around 200 Hz An initiative of drtbalu's otolaryngology online
Glottal fry • Low frequency phonation • In this type of vocal fold vibration closed phase is longer when compared with that of open phase • The vocal fold mucosa and vocalis muscle vibrate in unison An initiative of drtbalu's otolaryngology online
Mucosal wave • Very important physiological parameter to be noted during vocal fold motion • It is the undulation that occurs over vocal fold mucosa • This wave travels in infero superior direction • The speed of this wave 0.5 – 1 m/sec • Symmetry of these waves between both sides should be evaluated. Even mild degrees of asymmetry is pathological An initiative of drtbalu's otolaryngology online
Methods of speech following Laryngectomy • Also known as alaryngeal speech • Esophageal speech • Electro larynx • TEP (Tracheo-oesophageal puncture) An initiative of drtbalu's otolaryngology online
Esophageal speech Alaryngeal speech An initiative of drtbalu's otolaryngology online
Contd… • All pts. Develop some degree of esophageal speech following Laryngectomy • All alaryngeal speech modalities are compared with this modality • Till 1970’s this was the gold standard for all other post Laryngectomy speech rehabilitation procedures An initiative of drtbalu's otolaryngology online
Esophageal speech - Physiology • Air is swallowed into cervical esophagus • This swallowed air is expelled out causing vibrations of pharyngeal mucosa • These vibrations along with articulations of tongue cause speech to occur • The exact vibrating portion of pharynx is the pharyngo-oesophageal segment • The vibrating muscles and mucosa of cervical oesophagus and hypopharynx cause speech An initiative of drtbalu's otolaryngology online
Oesophageal speech – PE segment • This segment is made up of musculature and mucosa of lower cervical area (C5-C7 segments). • Vibration of this segment causes speech in pts. Without larynx • Cricopharyngeal area is important • Cricopharyngeal spasm in these pts. Can lead to failure in developing Oesophageal speech • Cricopharyngeal myotomy may help these pts. in developing Oesophageal speech An initiative of drtbalu's otolaryngology online
Pumping air into cervical oesophagus • Injection method • Inhalational method An initiative of drtbalu's otolaryngology online
Injection method • Enough positive pressure is built inside oral cavity to force air into cervical oesophagus • Lip closure and tongue elevation against palate causes increase intraoral pressure • Air is injected into the cervical oesophagus by voluntary swallowing • This method is also known as tongue pumping / glossopharyngeal press / glossopharyngeal closure • This method is really useful before uttering plosives / fricatives / affricatives An initiative of drtbalu's otolaryngology online
Inhalational method • Uses the negative pressure used in normal breathing to allow air to enter cervical oesophagus • Air pressure in the cervical oesophagus below Cricopharyngeal sphincter is the same negative pressure as that of thoracic cavity • Pts. Learn how to relax Cricopharyngeal sphincter during inspiration allowing air to flow into cervical oesophagus as it enters the lungs • Pts. Are encouraged to consume carbonated drinks which facilitates air entry into cervical oesophagus helping in generation of Oesophageal speech An initiative of drtbalu's otolaryngology online
Esophageal speech - Advantages • Patient’s hands are free • No additional surgery / prosthesis needed. Hence no extra cost for the pt. • Pts. Get easily adapted to esophageal voice An initiative of drtbalu's otolaryngology online
Esophageal speech - Disadvantages • Nearly 40% of pts fail to develop esophageal speech • Quality of voice generated is rather poor • Pt. may not be able to continuously speak using esophageal voice without interruption. They will be able to speak only in short bursts • Significant training is necessary • Loudness / pitch control is difficult • Fundamental frequency of esophageal speech is 65 Hz which is lower than that of male and female frequencies An initiative of drtbalu's otolaryngology online
Esophageal speech development causes for failure • Presence of cricopharyngeal spasm • Presence of reflux esophagitis • Abnormalities involving PE segment – like thinning of muscle wall in that area • Denervation of muscle in the PE segment • Poorly motivated patient An initiative of drtbalu's otolaryngology online
Cricopharyngeal spasm • Cricopharyngealmyotomy • Botulinum toxin injection – 30 units can be injected via the tracheostome over the posterior pharyngeal wall bulge An initiative of drtbalu's otolaryngology online
Electrolarynx • These are battery operated vibrating devices • It is held in the submandibular region • Muscle contraction and changes in facial muscle tension causes rudiments of speech • Initial training to use this equipment should begin even before surgery An initiative of drtbalu's otolaryngology online
Electrolarynx - Types • Pneumatic – Dutch speech aid, Tokyo artificial speech aid • Neck • Intraoral type An initiative of drtbalu's otolaryngology online
Electrolarynx - Contd • Neck type is commonly used • Hypoesthesia of neck during early phases of post op period can cause difficulties • If neck type cannot be used intraoral type is the next preferred one An initiative of drtbalu's otolaryngology online
Intraoral artificial larynx • Intraoral cup should form a tight seal over the stoma. There should not be any air leak • Oral tip should be placed in the oral cavity • Pts exhaled air rattles the cup placed over the stoma • Changes in exhaled pressure can vary the quality of sound generated An initiative of drtbalu's otolaryngology online
Electrolarynx - advantages • Can be easily learnt • Immediate communication is possible • Additional surgery is avoided • Can be used as a interim measure till the patient masters the technique of esophageal speech or gets a TEP inserted An initiative of drtbalu's otolaryngology online
Electrolarynx - Disadvantages • Expensive to maintain • Speech generated is mechanical in quality • Difficult while speaking over telephone An initiative of drtbalu's otolaryngology online
Types of voice restoration surgeries • Neoglottic reconstruction • Shunt technique An initiative of drtbalu's otolaryngology online
Neoglottis procedure • Performing trachea hyoidopexy • This can restore voice function in alaryngeal patients • Abandoned due to increased incidence of complications like aspiration An initiative of drtbalu's otolaryngology online
Shunt technique • Developed by Guttmann in 1930 • Involves creation of shunt between trachea and esophagus • Lots of modifications of this procedure is available, Basic principle is the same • Aim is to divert air from trachea into the esophagus An initiative of drtbalu's otolaryngology online
Types of shunts • High trachea-esophageal shunt (Barton) • Low trachea-esophageal shunt (Stafferi) • TEP shunts (Guttmann) An initiative of drtbalu's otolaryngology online
Causes of failure of shunt procedure • Aspiration through the fistula • Closure of the fistula • To avoid these problems prosthesis was introduced An initiative of drtbalu's otolaryngology online
Types of Prosthesis An initiative of drtbalu's otolaryngology online
TEP • Was first introduced by Blom and Singer in 1979 • One way silicone valve is introduced via the fistula • This valve served as one way conduit for air into esophagus while preventing aspiration • This prosthesis has two flanges, one enters the esophagus while the other rests in the trachea. It fits snugly into the trachea-esophageal wound • Indwelling prosthesis have more rigid flanges when compared to that of non indwelling ones • A medallion ring is attached to the non indwelling prosthesis to prevent aspiration An initiative of drtbalu's otolaryngology online
Types of TEP • Primary TEP – Performed during total laryngectomy • Secondary TEP – Performed 6 months after surgery An initiative of drtbalu's otolaryngology online
Anatomical structures TEP • TEP is performed in midline (Less bleeding) • Structures that are penetrated during TEP - membranous posterior wall of trachea, esophagus and its 3 muscle layers and esophageal mucosa • Interconnecting tissue in the trachea-esophageal space An initiative of drtbalu's otolaryngology online
Advantages of TEP • Can be performed after laryngectomy / irradiation / chemotherapy / neck dissection • Fistula can be used for esophago-gastric feeding during immediate PO period • Easily reversible • Speech develops faster than esophageal speech • High success rate • Closely resembles laryngeal speech • Speech is intelligible An initiative of drtbalu's otolaryngology online
Disadvantages of TEP • Pt should manually cover the stoma during voicing • Good pulmonary reserve is a must • Additional surgical procedure is needed to introduce it • Posterior esophageal wall can be breached • Catheter can pass through the posterior wall An initiative of drtbalu's otolaryngology online
TEP – Patient selection • Motivated patient • Patient with stable mind • Patient who has understood the anatomy & physiology of the process • Patient should not be an alcoholic • Good hand dexterity • Good visual acuity • Positive esophageal air insufflation test • Patient should not have pharyngeal stricture / stenosis • Stoma should be of adequate depth and diameter • Intact trachea-esophageal wall An initiative of drtbalu's otolaryngology online
Contraindications of TEP • Extensive surgery involving pharynx, larynx with separation of trachea-esophageal wall • Inadequate psychological preparation • Patient with doubtful ability to cope up with prosthesis • Impaired hand dexterity • Suspected difficulty during PO irradiation An initiative of drtbalu's otolaryngology online
Primary - TEP • Hamaker first performed in 1985 • Primary TEP should be attempted where ever possible • In this procedure puncture is performed immediately after laryngectomy and prosthesis is inserted • Prosthesis of sufficient length should be used An initiative of drtbalu's otolaryngology online
Primary TEP - Advantages • Risk of separation of trachea – esophageal wall is minimized • Tracheo – esophageal wall is stabilized to some extent by the prosthesis • Flanges of prosthesis protects trachea from aspiration • Stomal irritation is less • Patient becomes familiar with prosthesis immediately following surgery • Post op irradiation is not a contraindication An initiative of drtbalu's otolaryngology online
Primary TEP - Procedure • Because of exposure following laryngectomy it is easy to perform • Ideally performed before pharyngeal closure • Puncture is performed through pharyngotomy defect • Ryles tube can be introduced via the fistula to provide gastric feeding in the post op period An initiative of drtbalu's otolaryngology online
Secondary TEP • Usually performed 6 weeks following laryngectomy • This allows pt time to develop esophageal speech • Area of fistula identified using rigid esophagoscope • Prosthesis can be inserted immediatly An initiative of drtbalu's otolaryngology online
Modified secondary TEP procedure • Performed under local anesthesia • Patient placed in recumbent position with mild extension of neck with a shoulder roll • Tracheostomy tube is removed • 12 0 clock position of tracheostoma visualized and infiltrated using 2% xylocaine with 1 in 100,000 adrenaline • Yanker’s suction tube is inserted into the oral cavity till it hitches against 12-0 clock position of tracheostome • This area is incised using 11 blade and widened using curved artery forceps • Blom singer prosthesis is then introduced through this fistula An initiative of drtbalu's otolaryngology online
12 – 0 clock position of tracheostoma An initiative of drtbalu's otolaryngology online