Download

1 / 6
0 likes | 1 Views
A foot and ankle surgeon combines surgical skill with compassionate care to help you walk, run, and live with less pain and more confidence.

E N D
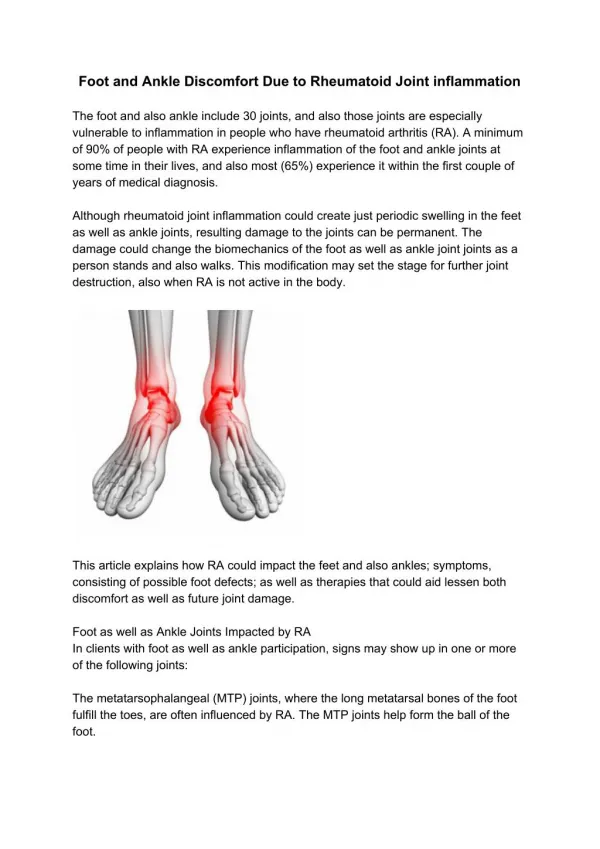
A well aligned foot is a quiet workhorse. When the bones stack correctly, the tendons fire in rhythm, and the joints glide, you do not notice each step. When alignment is off, every joint above the ankle, from the knee to the lower back, negotiates the compromise. I have seen patients who came in for “hip trouble” that traced back to a collapsing arch, and teenagers sidelined from sport because a subtle torsion in the hindfoot changed their sprint mechanics. Alignment is not a cosmetic nicety. It is a mechanical truth that dictates how you load the ground and how the ground loads you. Foot and ankle alignment surgeons focus on this mechanical truth. We look beyond the painful spot to the forces that created it. Whether you are searching for a foot and ankle surgeon near me or you simply want to understand what goes into restoring a natural gait, this is the landscape: anatomy, diagnostics, conservative care, and when needed, precise surgical correction that respects biology and biomechanics. What alignment means when you walk Gait is a coordinated series of controlled falls. The heel strikes, the foot accepts load, the arch stores energy, and the forefoot pushes you forward. In a healthy stride, the heel bone (calcaneus) sits under the leg, the subtalar joint allows predictable pronation and supination, the midfoot locks and unlocks at the right moments, and the first ray plants firmly so the calf can translate muscle pull into forward motion. Misalignment disturbs this sequence. A heel that drifts outward places the knee in valgus and stresses the medial ankle. A forefoot that is varus nods inward and forces chronic overpronation. A collapsed arch loses spring and transfers work to the plantar fascia and posterior tibial tendon. Over time, cartilage in the ankle and midfoot fails under asymmetric loads. The patient experiences pain, swelling after activity, frequent sprains, or a persistent sense that the foot is “not stable.” When I evaluate gait, I think in terms of levers, springs, and hinges. The foot is all three at different points in the step. The job of a foot and ankle alignment surgeon is to restore the geometry so the levers are efficient, the springs store elastic energy instead of burning it off as pain, and the hinges move without grinding. Who does this work and how they differ Patients often ask whether they should see a foot and ankle orthopedic surgeon or a foot and ankle podiatric surgeon. Both can be excellent choices. The titles reflect training paths, not a strict division of capability. Orthopedic surgeons complete medical school followed by an orthopedic residency, then a foot and ankle fellowship. Podiatric surgeons complete podiatric medical school, a surgical residency focused on the foot and ankle, often with fellowship training. What matters most is experience with alignment procedures, board certification, volume of cases, and an approach that blends conservative therapy with surgical judgment. Within the specialty there are focused roles. A foot and ankle trauma surgeon deals with fractures and dislocations. A foot and ankle sports injury doctor manages ligament tears and cartilage injuries in athletes. A foot and ankle arthritis specialist treats joint degeneration with joint-sparing osteotomies, fusions, or joint replacement. A foot and ankle deformity surgeon addresses flatfoot, cavus, bunions, hammertoes, and complex congenital issues. Many of us overlap these roles, but knowing the surgeon’s emphasis helps you match your problem to the right hands. Common alignment problems I see in clinic
Flexible flatfoot in adolescents and adults sits at the top of the list. The hindfoot tilts into valgus, the arch collapses, and the forefoot compensates with abduction. Early on, a custom orthotic and targeted strengthening quiet the symptoms. If the posterior tibial tendon fails or arthritis sets in, surgical reconstruction becomes the durable solution. Cavus foot is the opposite alignment, with a high rigid arch and a heel that often tilts into varus. These patients sprain easily and develop peroneal tendon problems. They also overload the lateral ankle and fifth metatarsal. Realigning the heel and balancing the forefoot can transform an ankle that rolled every month into one that feels planted. Chronic ankle instability usually starts after repeated sprains. Ligaments stretch, and the talus translates excessively under load. A foot and ankle ligament specialist evaluates not only the lateral ligaments but also the alignment that invites sprains. Correcting a varus heel without stabilizing the ligaments fails, and tightening ligaments without addressing the heel varus leads to recurrence. The fix is often both. Forefoot deformities like bunions and hammertoes are alignment problems at a smaller scale. A foot and ankle bunion surgeon chooses among dozens of osteotomies to align the first ray and restore balanced push-off. With hammertoes, we target the vectors on each phalanx and the pull of the flexor and extensor tendons so toes sit straight and bear load without corns or ulcer risk. Post-traumatic deformity after fractures is another frequent referral. A foot and ankle fracture specialist may see a calcaneus that healed in malalignment. The heel points outward and the subtalar joint is stiff, so every step hurts. Realignment can be more impactful than simply fusing a painful joint in its current, faulty position. How a careful evaluation prevents wrong turns There is no shortcut to a good foot and ankle exam. I ask about work demands, sport, terrain, shoes, and the hour of the day when pain rises. A marathoner with lateral ankle pain at mile 18 is a different problem than a teacher whose arch aches by lunchtime. I look at old orthotics and worn shoe patterns. Heel wear that is asymmetric or a forefoot imprint that shows excessive pressure on the second and third metatarsal heads tells me the compensation pattern. On exam, I check hindfoot alignment standing and from behind. I assess whether the heel inverts on heel rise, which indicates posterior tibial function. The Silfverskiöld test, which distinguishes gastrocnemius from soleus tightness, guides whether a calf lengthening could help. I compare forefoot to rearfoot alignment in subtalar neutral and note rigidity. I palpate the peroneal and posterior tibial tendons for crepitus or tenderness and test ankle ligament integrity with anterior drawer and talar tilt. Imaging is tailored. Weight bearing X-rays show alignment under load. A standing hindfoot alignment view quantifies varus or valgus. MRI helps for tendon tears, osteochondral lesions, and subtle stress injuries. CT shines with complex deformity and allows us to model osteotomy planes. Motion analysis is available in some centers and can reveal timing issues a static exam misses, especially in athletes. The final step is patient specific goal setting. A foot and ankle pain doctor treating a warehouse worker must prioritize durability on concrete, while a foot and ankle sports surgeon working with a sprinter has to respect return to sport timelines and the athlete’s need for explosive push-off. The plan shifts accordingly.
When nonoperative care is the best medicine Many alignment issues improve without surgery. This is not a defeat. It is a measured choice that respects tissue healing and functional adaptation. Targeted physical therapy builds intrinsic foot strength and restores ankle proprioception. A skilled therapist can retrain gait to reduce knee hyperextension that often accompanies flatfoot collapse. Gastrocnemius stretching changes forefoot load and is often overlooked. Custom orthoses are tools, not crutches. For flexible flatfoot, a semi rigid device with medial posting supports the arch and improves subtalar mechanics. For cavus feet, a softer top cover with lateral forefoot posting reduces lateral overload. Bracing plays a role for posterior tibial tendon dysfunction and chronic ankle instability. A lace up or semi rigid brace during sport can dramatically reduce sprains while rehab strengthens the peroneals and improves balance. Activity modification is not a sentence to inactivity. I often shift a runner to cycling and pool workouts for eight to twelve weeks while we unload inflamed tissue, then rebuild miles on a cadence plan that respects tissue capacity. Topical anti inflammatories and short courses of oral medication reduce pain to allow participation in therapy. Injections have a place, mainly for joint inflammation or recalcitrant plantar fasciitis. I am cautious with corticosteroids around tendons, especially the Achilles and posterior tibial tendon, due to rupture risk. Biologic injections are evolving. Evidence is mixed, and I have seen benefits in select cases of mild tendinopathy when combined with a strict rehab protocol, but it is not a panacea. Choosing surgery and choosing the right surgery Surgery enters the conversation when pain persists despite appropriate care, deformity progresses, or the alignment is rigid and functionally limiting. The decision turns on three questions. Can we correct alignment to a durable, plantigrade foot. Can we do it while preserving as much motion as possible, or is fusion the best way to remove pain from an arthritic joint. Will the rehabilitation fit the patient’s life and goals. In flatfoot reconstruction, a foot and ankle reconstructive specialist may combine procedures to address each segment. A medializing calcaneal osteotomy shifts the heel under the leg to correct valgus. A lateral column lengthening restores the arch and reduces forefoot abduction. If the posterior tibial tendon is torn, we transfer the flexor digitorum longus to restore inversion power. If the forefoot is supinated relative to the midfoot after hindfoot correction, we add a plantarflexion osteotomy of the medial cuneiform. Each step is measured intraoperatively with fluoroscopy and by checking the foot on a simulated plantigrade load. For cavus, a foot and ankle correction surgeon often performs a lateralizing calcaneal osteotomy to bring the heel out of varus. A dorsiflexion osteotomy of the first metatarsal reduces overload under the lateral column. Tendon transfers, such as moving some peroneus longus power to the brevis, balance forces. The goal is to distribute load evenly and prevent the next sprain. Chronic ankle instability responds well to an anatomic ligament repair, like a modified Broström procedure, sometimes augmented with internal bracing. The alignment surgeon looks up the kinetic chain to confirm there is no unaddressed hindfoot varus that would sabotage the repair. If present, we correct both. Arthritis decisions require nuance. In isolated ankle arthritis with preserved alignment and significant pain, a foot and ankle joint replacement surgeon may recommend total ankle arthroplasty to preserve motion, especially in patients over 55 with lower activity demands and good bone quality. In severe deformity, neuropathy, or heavy laborers, a fusion can be the more reliable workhorse. A well aligned fusion, with the foot plantigrade and the heel slightly valgus, can provide decades of pain relief and strong push-off through the midfoot. Minimally invasive techniques have expanded our toolkit. A foot and ankle minimally invasive surgeon can perform percutaneous calcaneal osteotomies through small incisions, decreasing soft tissue irritation and potentially speeding wound healing. MIS bunion corrections reduce scars and soft tissue disruption. These approaches still demand the same attention to axes and angles. Smaller incisions do not excuse imprecise alignment. The day of surgery and the months that follow Surgical success hinges on the strategy you execute before and after the operating room. I prepare patients with two weeks of prehab when possible. Learning to use crutches, arranging a knee scooter, setting up a first floor living space, and precooking meals sound mundane. They are the difference between safe recovery and a preventable fall.
Anesthesia choice varies expert ankle surgeon in NJ by procedure and patient. Regional blocks can provide 12 to 24 hours of pain relief and significantly reduce opioid needs. I am specific about elevation and swelling control. For the first 72 hours, toes above the nose is not an exaggeration. The foot and ankle are distant from the heart and love to swell. Controlling that swelling protects the incision, reduces pain, and speeds the first steps of rehab. Weight bearing protocols depend on the work done. Osteotomies and fusions usually require six to eight weeks of protected weight bearing in a cast or boot. Tendon transfers and ligament repairs need time to heal before loading them. We schedule milestones: suture removal at two weeks, X-rays at six to eight weeks, transition to a boot, and initiation of physical therapy. Return to running after realignment is often at four to six months, with full return to sport after six to nine months depending on the complexity. Rehabilitation is not generic. A foot and ankle rehabilitation surgeon works closely with therapists to sequence range of motion, scar mobilization, swelling management, and progressive strength. We prioritize single leg balance early to restore proprioception. Calf strength often takes the longest. Patients are tempted to overstride when running resumes. Cadence drills and metronome runs prevent reloading old patterns that caused trouble. What results look like in real life Numbers matter, but stories clarify. A 42 year old nurse with progressive flatfoot could barely finish a 12 hour shift. She had tried bracing and orthoses for a year. Her hindfoot valgus measured 12 degrees. We planned a medializing calcaneal osteotomy, FDL transfer, and gastrocnemius recession. At eight months, she returned to full shifts with orthotic support in a stable shoe. She sent a picture from a weekend hike two months later. Not a sprint, but a life restored to motion. Another patient, a 19 year old collegiate volleyball player, sprained her ankle six times in a season. Exam showed laxity and a subtle cavus with a varus heel. We performed a lateralizing calcaneal osteotomy and a Broström ligament repair. She followed a strict rehab plan and returned to play at eight months. Two seasons later, no sprains, and video showed her landing mechanics were cleaner. A 65 year old contractor with end stage ankle arthritis and significant varus had pain with every step. Given his heavy labor and the deformity, we chose a tibiotalar fusion with calcaneal realignment. He was back on light duty at four months and full duty at nine months. He notices less dorsiflexion when going downhill, but he can work a full day without swelling and pain. A joint replacement might have preserved motion but was unlikely to survive his occupational load and the deformity without early failure. Trade offs, risks, and realistic expectations Every procedure carries risk. Wounds on the medial hindfoot are slow to heal in smokers and diabetics. Nerves such as the sural and saphenous run close to osteotomy sites and require careful handling. Nonunion rates for fusions vary by joint and patient factors. Tendon transfers do not restore original anatomy, they reassign force vectors. Most patients adapt well, but top end power in a specific movement may change. Communication about these realities builds trust. There are also trade offs in the clinic. Bracing helps but can weaken muscles if used all day every day without structured strengthening. Orthotics that are too rigid cause new calluses. A foot and ankle pain specialist must balance relief with the long game of tissue health. Recovery takes longer than most patients expect. Bone heals in weeks, but neuromuscular patterns take months. The brain needs reps to trust a newly aligned foot. Celebrating small wins helps. The first painless grocery trip, the first stairs without a handrail, the first jog on a soft track, each milestone matters. Shoes, surfaces, and the quiet details that carry you Footwear is a lever you control daily. After realignment, most patients do best in shoes with a stable heel counter, mild medial or lateral posting depending on the correction, and a forefoot rocker that reduces stress under the metatarsal heads. Super soft, high stack shoes feel pleasant but can be unstable for a recently reconstructed foot. On the job, a well cushioned, supportive work boot beats a minimal sneaker on concrete. Orthotics remain helpful, but the goal is not dependence. For many, a custom device lives in work shoes, while a softer over the counter insert suffices for casual wear. Runners benefit from gradual reintroduction of miles with a cadence target of 165 to 180 steps per minute, which reduces peak ground reaction forces and helps form.
Surfaces matter. Early return to impact should be on a track or turf, not a cambered road that forces one foot into chronic inversion. Trail runners with prior instability should learn to read terrain and place the foot under the center of mass rather than reaching. Small habits prevent big setbacks. Finding the right partner for your problem Patients often search for a foot and ankle specialist near me, foot and ankle doctor near me, or a foot and ankle orthopedic doctor without a clear sense of what to ask. Experience, outcomes, and communication style matter more than a single title. Ask how many procedures like yours the surgeon performs each year. Inquire about complication rates, reoperation rates, and typical timelines back to work or sport. A foot and ankle clinical specialist should be comfortable explaining why your plan includes or avoids certain steps. Check whether the practice includes a foot and ankle podiatry surgeon and a foot and ankle orthopedic surgeon working together, especially if your case involves both soft tissue and complex bone correction. Teams that include a foot and ankle biomechanics specialist, a foot and ankle movement specialist for gait retraining, and therapists familiar with lower extremity reconstruction often deliver smoother care. For pediatric issues, look for a foot and ankle pediatric specialist experienced in growth plate considerations. Below is a compact set of questions that often clarifies the path forward. What is the specific alignment problem in my foot or ankle, and how does it change my gait. Which nonoperative options have the best chance of success for my case, and over what timeframe. If surgery is recommended, what procedures correct each component of my deformity, and what are the key risks. How long will I be non weight bearing, when can I return to work or sport, and what does the rehab plan look like week by week. How will we measure success, and what is the plan if a milestone is not met on time. Special situations that deserve extra attention Diabetes and neuropathy change tissue quality and sensation. A foot and ankle nerve specialist and a foot and ankle bone specialist will consider protective alignment that reduces pressure points and ulcer risk. For Charcot arthropathy, the goal is a plantigrade, braceable foot, often with staged reconstruction and a longer healing timeline. Rheumatoid arthritis creates multi joint involvement and ligament laxity. A foot and ankle arthritis specialist balances joint preserving procedures with selective fusions to create a painless, functional platform. Medical management by a rheumatologist is essential to reduce flare risk around surgery. High level athletes place unique demands on reconstructions. A foot and ankle sports surgeon coordinates with strength coaches to sequence return to cutting and jumping. Objective measures like single leg hop testing, force plate analysis, and isokinetic strength ratios guide clearance. The bar is higher, and the detail work shows in late game fatigue mechanics. Older adults need practical plans. A foot and ankle chronic pain doctor may emphasize pain control, balance training, and targeted injections over large reconstructions, unless the deformity prevents safe ambulation. When surgery is right, simplifying the operative plan to the fewest effective steps can reduce risk without sacrificing function. The role of precision in imaging, planning, and execution Modern alignment work benefits from 3D imaging and patient specific planning when appropriate. Weight bearing CT allows us to visualize deformity under load. For complex cases, we can plan osteotomy cuts and simulate corrections. Intraoperative fluoroscopy is standard, but we do not let images dictate reality without checking the foot on a simulated plantigrade position. The eye and the hand must agree with the screen. Hardware choice is practical. Low profile plates minimize irritation, and screws should compress where needed without crossing joints unnecessarily. In revision work, a foot and ankle corrective surgery expert anticipates poor bone quality and plans for biologic augmentation. The principle remains consistent: achieve alignment, achieve stability, protect the biology, and then let time and rehab do their part. What a good outcome feels like, not just what it looks like
On X-ray, success is angles within accepted ranges. In life, success is walking a dog after dinner without thinking about each step, jogging a 5K at a comfortable pace, finishing a workday on concrete with legs foot and ankle surgeon NJ that feel merely tired rather than throbbing. Patients describe a shift from guarding to confidence. They stop planning routes around elevators. They start saying yes to invitations that require standing. The most gratifying moment comes when the gait looks quiet. The head rides level, the pelvis rotates smoothly, and the foot lands under the center of mass with a soft, deliberate contact. That is the sign the architecture is right and the neuromuscular system trusts it. Final thoughts from the clinic Alignment work lives at the intersection of anatomy, physics, and habit. It takes clear diagnosis, disciplined nonoperative care, and, when indicated, a thoughtful operation done by a foot and ankle alignment surgeon who respects both bone and soft tissue. It also takes a patient who understands the process and commits to recovery. If your foot collapses as the day wears on, if your ankle feels ready to roll on uneven ground, if you have tried generic inserts without real change, an experienced foot and ankle care specialist can map the problem and chart the path back. Whether your solution is a new set of exercises and a better brace from a foot and ankle care provider, or a staged reconstruction by a foot and ankle surgical specialist, the aim is the same: a stable, efficient, pain controlled gait that disappears into the background of a well lived day.