Download
1 / 25
250 likes | 393 Views
Airway’s infections Epidemiology - In children < 5 years of age. 50 % of all diseases are acute airway’s infections - In children 5-12 years of age 30 % of all diseases are acute airway’s infections

E N D
Airway’s infections • Epidemiology • - In children < 5 years of age. 50 % of all diseases are acute airway’s infections • - In children 5-12 years of age 30 % of all diseases are acute airway’s infections • - Most of the infections are in the upper airways, only 5 % are in the larynx and or in the lower airways • The natural history of the disease depends of • the pathogen (microbe), • the host, • the environment
Localisation of the acute airways’ inflammations • Upper airways’ inflammation • Laryngo-tracheo-bronchitis (croup), epiglottitis • Acute bronchitis • Acute bronchiolitis • Pneumonia
Infectious agents of the upper respiratory tract I. Viruses Respiratory syncytial virus (RSV): bronchiolitis, pneumonia, croup, bronchitis Parainfluenza viruses: croup syndorma, bronchitis, bronchiolitis Influenza virus: in epidemics Adenoviruses: pharyngitis, pharyngoconjunctivits Rhinoviruses Coronaviruses:rhinitis, common cold Coxsackieviruses A and B: nasopharyngitis
Infectious agents of the upper respiratory tract II. Mycoplasma pneumoniae: pharyngotonsilitis, otitis media, pneumonia, bronchitis Bacterial causes: ‘A” group streptococci, corynebacterium diphteria, Neisseria meningitidis, N gonorrhoeae, haemophilus influenzae, streptococcus pneumoniae (pneumococcus), staphylococcus aureus
Signs of • inclination for frequent infections • Too frequent infections • Age/year Mean Maximum • 1 6,1 8,7 • 1-2 5,7 8,7 • 3-4 4,7 7,6 • 5-9 5,5 8,1 • 10-14 2,7 4,9 • Longer (> 4-5 days) and more serious infection than the usuals • Bacterial second line infection • Complications: otitis, sinusitis, pneumonia • Multiorgan infections • Failure to thrive
Bacterial infection is probable: • The discharge on the mucous membrane is purulent • Polymorpho-nuclear granulocytes’ number is high in the peripherial blood • Positive bacterial laboratory findings (from throat or sputum) • The regional lymphnodes are swollen and painful • Blood sedimentation rate is high • There is no viral epidemy
Infection risk factors in the host • Preterm babies (< 1 year) • Age less than 1 year (< 6 months in bronchiolitis) • To be a boy • Inborn errors of the immune system • Congenital heart defects • Lack of mother milk
Environmental factors • Family care (+) • Smoking in the family (-) • More than one child (-) • Good socio-economic situation (+) • Polluted environment (-)
The aetiology of common flu Antigen types Per cent of probability Rhinovirus100 types 30-40 % Coronavirus 3 types > 10 % Parainfluenzavirus 4 types RSV2 types Influenza 3 types 10-15 % Adenovirus 47 types 5 % Others (enterovirus, morbilli, varicella, rubeola) 5 % Unknown viruses 25-30 % A-group beta-haemolytic Streptococci 5-10 %
Upper airway diseases Nasopharyngitis acuta: fever, headache, dry throat, coughing, nasal discharge, frequent conjunctical inflammation, stuffed nose (feeding problems in infants) Tonsillo pharyngitis acuta: red mucous membrans, swollen families, swollen tonsils, swollen lymphnodes in the neck, fever, pain Therapy: antipyretics, antiphlogistic nasal drops, enough fluid intake, Bacterial infection: penicillin, enythromycin (10 days) Non streptococcal infection: amoxycillin, macrolides, cephalosporins Complications: otitis media acuta, peritonsillar retropharyngeal abscess Sinusitis acuta Febris rheumatica, glomerulonephritis (now rare)
Pathogenesis of tonsillopharyngitis Pathologic agents Features Per cent Viruses (see before) 35-40 % + Coxsackievirus herpangina < 1 % EBV + CMVmononucleosis inf. < 2 % HIV primer HIV infection < 1 % Bacterial Streptococci pyogenes 15-30 % Beta-haemolytic Streptococci 5-10 % Other bacteria < 5 % Unknown 20-30 %
Complications of upper airway inflammations Otits media Mastoiditis acuta Paranasal sinusitis Peritonsillar, retropharyngeal infiltration, abscessus Poststreptococcal diseases: rheumatic fever, glomerulonephritis Croup cyndrome Acute epiglottitis Acute infectious laryngitis Acute laryngo-tracheo-bronchitis Acute spasmodic laryngitis
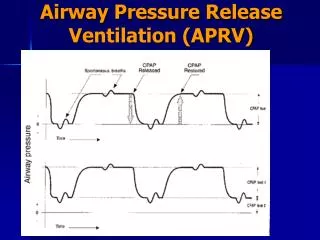
Laryngitis subglottica (croup syndrome) Very frequent Aetiology:viral, bacterial, mycoplasma non infective: inclination, alllergic (?) Croup score: stridor, cough, dyspnoe, cyanosis, inspiratoric sound, jugular dystraction (0-1-2) 3-5 moderate 6 or more serious Therapy:cold vaporization epinephrin (racem) vaporized steroid (systemic or vaporized) antibiotics (if proved bacterial aetiology) intubation, artificial ventillation
Acute bronchitis, tracheo bronchitis Cough, sputum, bronchial noises, substernal dyscomfort, low grude fever Coarse and fine moist rales and rhonchi Etiology: viral or bacterial Therapy: symptomatic (to be at home, antipyretics, fluid intake) Bacterial aetiology proven: antibiotics
Pneumonia I. • Actiology: viral, bacterial, fungal • Clinical manifestations: lobar, lobular, broncho-alveolar, interstitial • community acquired pneumonia • nosocomial (hospital) acquired pneumonia • Bacterial: • Typical pneumonia: streptococcus pneumoniae • Haemophylus influenzae B type (vaccination!) • Streptococcus B Group: neonatology • Seldom: staphilococcus auerus, pyogenes, legionella • Atypical: Mycoplasma pneumoniae • Chlamydia pneumoniae • Neonates: Chlamydia trachomatis, Ureaplasma, Uraeliticum
Pneumonia II. • Viral: RSV, influenza, adenovirus, rhinovirus, enterovirus • VZV, CMV, HSV (immuncompromised host) • Fungal: immuncompromised host • Protozoons: Pneumocystic carinil (AIDS, immuncompromised host)
Pneumonia III. Clinical signs: fever, cough, malaise, sputum, dyspnoe, cyanosis, tachypnoe Physical signs: duffness of percussion pneumonia bronchial breath sounds X ray (sonography: pleural effusion CT and MR: abscess, mediastinum problems Laboratory signs: BSR, CRP, blood smear Actiology: haemoculture BAL, Pleural drainage (if effusion) induced sputum (?)
candidiasis aspergillosis patients with leukaemia
Therapy of pneumonia • symptomatic • antibiotics • - based on aetiology and resistance • - based on empirical facts: • macrolids • Cephalosporins • aminoglycosids • HSV/VZV: acyclovir. • CMV: gancyclovir • RSV: ribavirin
Acute nasophayngitis: Aetiology:viruses, mycoplasma pneumonieae, bacterial mycotic Epidemilogy Clinical manifestations Therapy:aspecific, antiinflammatory drugs, nasal drops and suction Acut pharyngitis, pharyngo-tonsillitis: Aetiology:viruses, beta-haemolytic streptococcus (group A) H. influenzae Epidemiology Clinical manufestations Treatment:aspecific, penicillin, erythromycin
The pathogens I. Virus RS virus: acute bronchiolitis in infants and toddlers (80 %) croup (12 %), bronchitis (15 %), pneumonia (30 %) Parainfluenza virus: laryngo-tracheo bronchitis, pneumonia Influenza virus: upper airway disease anywhere inflammation in the airways Rhinovirus: common cold, rhinitis, bronchitis Adenovirus: mostly upper airways’ disease serious pneumonia with serious late consequences Coxsacie and echovirus: mostly upper airway disease
The pathogens II. Bacteria Streptococcus pneumoniae: often in pneumonia Haemophilus influenzae B type: epiglottitis (!), pneumonia, otitis Staphylococcus aureus: pneumonia, pleuritis in infants and toddlers β-haemolytic streptococcus’ mostly upper airway inflammation, tonsillitis Mycoplasma pneumoniae: pneumonia in bigger children Chlamydia trachomatis: pneumonia in infants Chlamydia pneumoniae: bronchitis, seldom pneumonia Bronchamella catarrhalis: otitis, sinusitis in children