Download
1 / 6
60 likes | 519 Views
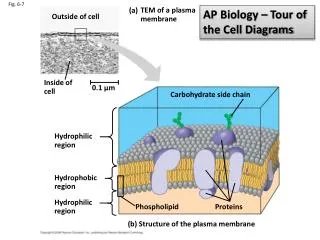
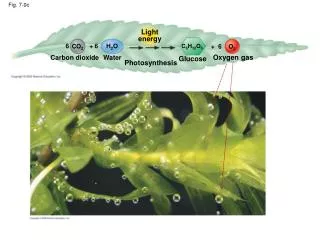
Fig.7.Estenosis ureteral tras transplante renal. A. 1 er Nefrostograma estenosis ureteral larga. C. Nefrostograma de control estenosis residual . B. 1 a dilatación con PCB. D. Nueva dilatación con PTA. E. Nefrostograma final. DISCUSIÓN II.

E N D
Fig.7.Estenosis ureteral tras transplante renal A. 1er Nefrostograma estenosis ureteral larga C. Nefrostograma de control estenosis residual B. 1a dilatación con PCB D. Nueva dilatación con PTA E. Nefrostograma final
DISCUSIÓN II • Nuestros resultados coinciden con lo expuesto en la literatura para PTA, pero el porcentaje de éxitos con PCB es menor a lo publicado; ésto podría explicarse por: • PCB se introdujo en nuestro departamento con posterioridad. • El grupo muestral de PCB es más pequeño y más reciente tiempo de seguimiento más corto: • Los dos últimos casos se siguieron sólo unos pocos meses, no incluyéndose en los resultados de permeabilidad a un año. • Suponiendo que hubieran sido permeables al año, la diferencia de permeabilidad PCB-PTA podría ser de un 5-10%, a favor de PCB. • En estenosis malignas, consideramos que los stents ureterales, con mejoras técnicas que prevengan complicaciones (migración, desgarro y obstrucción), pudieran y debieran ser de 1ª elección. • Son necesarios estudios que valoren la utilidad de desarrollar nuevos stents temporales para el tratamiento de estenosis benignas resistentes.
CONCLUSIÓN • Exponemos nuestra experiencia con 42 pacientes con estenosis ureterales postquirúrgicas, tratadas con dos métodos diferentes, uno convencional (PTA) y otro introducido más recientemente (PCB). • Los resultados iniciales de las dos técnicas son ligeramente mejores con PCB, pero al año de seguimiento, son superponibles. • Para clarificar mejor la diferencia, debemos aumentar el tiempo de seguimiento. • Otros estudios son necesarios con muestras de pacientes más grandes, para valorar si la diferencia entre los dos métodos es significativa.
REFERENCIAS I • Touiti D, Gelet A, Deligne E, Fassi-Fehri H, Benrais H, Martin X, et al. Treatment of uretero-intestinal and ureterovesical strictures by acucise balloon catheter. Eur. Urol. 2002; 42 (1): 49-55. • Bhayani S.B, Landman J, Slotoroff C, Figenshau R.S. Transplant ureter stricture: Acucise endoureterotomy and balloon dilation are effective. J. Endourol. 2003; 17 (1): 19-22. • Hafez K.S, Wolf J.S. JR. Update on minimally invasive management of ureteral strictures. J. Endourol. 2003; 17 (7): 453-464. • Chandhoke PS, Clayman RV, Stone AM, McDougall EM, Buelna T, Hilal N, et al. Endopyelotomy and endoureterotomy with the acucise ureteral cutting balloon device: preliminary experience. J. Endourol. 1993; 7(1): 45-51. • Catalá V, Solá M, Samaniego J, Martí T, Huguet J, Palou J, et al. CT findings in urinary diversion after radical cystectomy: postsurgical anatomy and complications. Radiographics 2009; 29 (2): 461-476. • Seseke F, Heuser M, Zöller G, Plothe K.D, Ringert R.H. Treatment of iatrogenic ureteral postoperative strictures with acucise endoureterotomy. Eur. Urol. 2002; 42: 370-375. • Atar E, Bachar GN, Bartal G, Mor E, Neyman H, Graif F, et al. Use of peripheral cutting balloon in the management of resistant benign ureteral and biliary strictures. J. Vasc. Interv. Radiol. 2005 ;16:241-245. • Bachar G.N, Mor E, Bartal G, Atar E, Goldberg N, Belenky A. Percutaneous balloon dilatation for the treatment of early and late ureteral strictures after renal transplantation: long-term follow-up. Cardiovasc. Intervent. Radiol. 2004; 27: 335-338.
REFERENCIAS II • Patel R.C, Newman R.C. Ureteroscopic management of ureteral and ureteroenteral strictures. Urol. Clin. N. Am. 2004; 31: 107-113. • Ravery V, de la Taille A, Hoffmann P, Moulinier F, Hermieu J.F, Delmas V, et al. Balloon catheter dilatation in the treatment of ureteral and ureteroenteric stricture. J. Endourol. 1998; 12 (4): 335-340. • Banner MP, Pollack HM, Rinq EJ, Wein AJ. Catheter dilatation of benign ureteral strictures. Radiology 1983; 147(2): 427-33. • Liatsikos EN, Kagadis GC, Karnabatidis D, Katsanos K, Papathanassiou Z, Constantinides C, et al. Application of self-expandable metal stents for ureteroileal anastomotic strictures: long term results. J Urol. 2007; 178(1):169-173. • Ganatra AM, Loughlin KR. The management of ureteral malignant obstruction treated with ureteral stents. J Urol. 2005;174(6): 2125-2128. • Atar E, Bachar GN, Eitan M, Graif F, Neyman H, Belenky A. Peripheral cutting balloon in the management of resistant benign ureteral and biliary strictures: long-term results. Diagn. Interv. Radiol. 2007;13(1): 39-41. • Cornud F, Chrétien Y, Hélénon O, Casanova J-M, Correas J-M, Bonnel D, et al. Percutaneous Incision of Stenotic Uroenteric Anastomoses with a Cutting Balloon Catheter: Long-term Results. Radiology 2000;214:358-362. • Juaneda B, Alcaraz A, Bujons A,Guirado L, Díaz JM, Martí J, et al. Endourological management is better in early-onset ureteral stenosis in kidney transplantation. Transplant Proc. 2005;37(9): 3825-3827.