Download
1 / 12
130 likes | 379 Views
in 5 minutes!?. Alarm Features starring the High Risk Diabetic Foot. Sue Robb Podiatrist Foot Health Service West Hertfordshire Community Health Services. The Diabetic Foot – when to refer. QOF screening – Who is high risk? Alert! ] refer to Foot Health Service

E N D
in 5 minutes!? Alarm Features starringthe High Risk Diabetic Foot Sue Robb Podiatrist Foot Health Service West Hertfordshire Community Health Services
The Diabetic Foot – when to refer • QOF screening – Who is high risk? • Alert! ] refer to Foot Health Service • Alarm ! ] urgent referral, & include Foot Health Service
Risk features of neuropathic foot QOF points • Warm foot, well-perfused, bounding pulses, distended veins due to a-v shunting • Sweating i skin dry/fissured • Distal (below knee) symmetrical sensory loss • Deformity, flexed toes, high arch, prominent met heads • High pressure points a callus
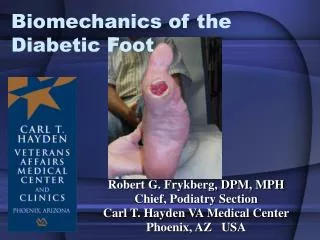
Neuropathic ulceration • Plantar metatarsal heads, apecies of toes • High vertical pressures • Ulcer covered/surrounded by callus, macerated by discharge • Usually painless – pain first sign infected • Good circulation – necrosis develops secondary to infection
Charcot arthropathy • Neuropathic osteoarthropathy - non infective destruction of bone • Affects patients with neuropathy • Acute phase mimics infection • Casting stabilisation / non-weight bearing essential • Weight bearing e ‘bag of bones’ appearance e ulcer from deformity
QOF points Neuroischaemic foot • Atrophic thin frail shiny skin • Diminished/absent foot pulses • Pallor on elevation • Rubor on dependency due to capillary dilatation • Intermittent claudication / rest pain, yet may be pain free • Unforgiving foot
Neuroischaemic ulceration • Ulcers on margins of feet associated with trauma and fragile micro circulation • Thin glassy callus or no callus • First sign? - skin discolouration that blisters • Pain may be due to infection or ischaemia
High risk - presence of any risk factor for ulceration. Refer to FHS + continue screening Risk factors for ulceration are Previous ulceration / amputation Neuropathy Absent/diminished pulses Deformity / LJM Callus Oedema Visual loss Self neglect / disability Identify high risk at screening No risk factors for ulceration =Low current risk Foot care education + annual screening. No FHS ref
Pre ulcerative callus Infection Sausage shaped toes “Beef chipolatas” Probe to bone <Osteomyelitis Look for signs of response to t/t in 3 days
Prevention of diabetic foot ulceration • Good glycaemic control essential • Education – improve foot care knowledge and behaviour • Daily foot check • Appropriate footwear • Timely vascular intervention • ‘High risk’ patients referred to Foot Health Service
‘Team’ working prevents problems • Early recognition and referral of the ‘at risk’ foot • Early detection and referral of ulceration, Charcot, severe infection, acute/critical ischaemia • ‘Shared care’ programme – diabetes team, GP, nurse, podiatry and patient
Thank you for listening ……Useful websites –www.diabeticfootjournal.co.ukwww.footindiabetes.orgwww.feetforlife.org