Download
1 / 23
240 likes | 434 Views
Minimal Requirements for Pediatric Cancer Units (PCU) in Developing Countries. AZIZA SHAD, MD Lombardi Cancer Center Georgetown University Hospital Washington DC,USA. Key elements of successful treatment of Pediatric cancer in Resource - Poor Countries. Identification of local needs

E N D
Minimal Requirements for Pediatric Cancer Units (PCU) in Developing Countries AZIZA SHAD, MD Lombardi Cancer Center Georgetown University Hospital Washington DC,USA
Key elements of successful treatment of Pediatric cancer in Resource - Poor Countries • Identification of local needs • Separate pediatric oncology unit • Twinning programs with recognized centers • Development of a multi-disciplinary health care team • Improvement in supportive care • Consistent availability of drugs • Subsidized travel and housing for families • Development of treatment protocols adapted to local conditions
Organization of a PCU1991 SIOP Guidelines • All children with cancer should be offered diagnosis, treatment, after care and follow-up • Special attention for adolescents and young adults up to the age of 20 • A PCU should provide centralized treatment for at least 50 new patients a year
Pediatric Cancer Units • A PCU should be a special unit • In a pediatric department • In a large oncology center • Multidisciplinary team • A PCU should be linked with a national or international multidisciplinary organization • Participate in new treatment through clinical trials • Research • Data management facilities should be available
Consensus Points from PODC Symposium, SIOP Berlin, 2008 • The 1991 guidelines are good, but may represent a standard that is still difficult to achieve in many developing countries, particularly in Africa and some parts of Asia • On the other hand, significant progress has been made in other parts of the world e.g. India, Brazil and several Middle East countries, necessitating addition of other elements for a ‘State of the Art’ PCU • The guidelines, therefore, needed revision.
Recommendations from PODC Symposium, SIOP Berlin, 2008 • All PCUs should be classified as Basic Level, Intermediate level and Advanced Level, based on their facilities and capability to provide patient care
Recommendations from PODC Symposium, SIOP Berlin, 2008 General Guidelines for All Levels: • The age range of patients served in a PCU can range from infancy through adolescence or even early adulthood (i.e. up until the age of 21 years) • Basic infection control practices e.g. good hand-washing policies, isolation of infectious cases, should be incorporated into all levels of PCU’s • All physicians involved in the diagnosis and care of cancer patients should have a working knowledge of palliative care including pain management.
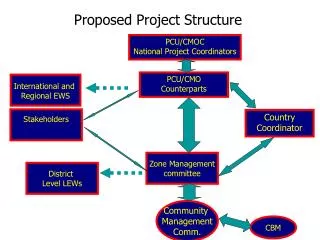
INCTR Pediatric Oncology Strategy Group Meeting Brussels, November 2008 • Over 20 pediatric oncologists, nurses, social workers and psychologists from Asia, Africa, Middle East, South America, Europe and USA • SIOP Recommendations used as baseline • INCTR Guidelines for Pediatric Oncology Units (POU)
INCTR Guidelines for Pediatric Oncology Units (POU) • All children, adolescents and young adults deserve age-appropriate diagnosis, treatment, aftercare and long term follow-up. • This is best offered in a dedicated Pediatric Oncology Unit (POU). • A POU should be situated in, or have an affiliation with a general hospital, pediatric departments or cancer center. • Depending on the extent of services offered, all POU’s can be divided into Level I, II or III.
General Guidelines for all Levels of POU’S • The age range of patients served in a POU can range from infancy through adolescence or even early adulthood (i.e. up until the age of 21 years) • Basic infection control practices (e.g. good hand-washing policies, isolation of infectious cases), should be incorporated into all levels of POUs • All POUs should be staffed by pediatric oncologists, or pediatricians who have had some formal training in pediatric oncology • All physicians involved in the diagnosis and care of cancer patients should have a working knowledge of palliative care including pain management.
Level I POU • A Level I POU is defined as a unit capable of diagnosing and delivering care for the most curable and least complicated pediatric oncology diagnoses (i.e. Hodgkin’s disease, non-Hodgkin’s lymphoma, ALL, and Wilm’s Tumor) • This POU should also have the capability of diagnosing and stabilizing patients with more complicated cancer diagnoses prior to transfer to a higher level POU.
Level I POU Facility and Infrastructure: • Level I POUs could be located in large cities (as one of several units) or small cities and towns (outside major metropolitan areas) where the POU might be the only center for treatment of non complicated cancers • Be located within or associated with a general hospital • Have capacity for both Inpatient and Outpatient care (ability to deliver chemotherapy for above mentioned tumors, provide antibiotics for fever and neutropenia, and transfusions) • Have the ability to communicate with all ancillary services (e.g. telephone, internet or pager) • Have a Chemotherapy Safety protocol and procedures to avoid chemotherapy errors and manage chemotherapy accidents (i.e., spills) • Have a hospital policy for the procurement, storage and accountability of drugs (usage, expiration dates, availability of stock) and other essential supplies needed for chemotherapy preparation and administration. A link with a central procurement agency may be needed in some countries.
LEVEL I POU Staff: • Pediatric oncologists or pediatricians with basic training in pediatric oncology • Nurses trained in basic pediatric care and care of the immunocompromised patient • Availability of a pathologist or interventional radiologist for fine needle aspirate/biopsy • Availability of a surgeon – preferably pediatric surgeon • Nursing staff should have a working knowledge of chemotherapy administration: i.e. placement of IV’s, administration of fluids and basic chemotherapy (i.e. Vincristine, Cyclophosphamide) • Pediatricians should have a basic, working knowledge of chemotherapy, its administration and side effects. This includes intrathecal chemotherapy • Pediatricians should be trained to do procedures (bone marrow aspiration/biopsy, spinal taps with intrathecal chemotherapy) and the interpretation of the results • ‘Round the Clock’ access to a pediatric oncologist /pediatrician and nursing should be available 7 days a week
Level I POU • Diagnostic Facilities: • Access to a basic laboratory (cross match, basic chemistry, bone marrow stain, and CBC) • Plain X-ray facility; optimally ultrasound capability • Have a close link to a higher level POU, which could accept patients with more advanced disease, confirm diagnosis, and recommend treatment • Availability of pathology services for diagnosis • Access to an accredited Blood Bank.
Level I POU • Support Services: • Emergency transportation for patients between institutions or for home. • Basic resuscitation equipment on site including wall or portable oxygen. • Adequate hand washing facilities and sinks. • Transportation for patient related activities.
Level I POU • Academic Activities: • Have a close link to a higher level POU, which could accept patients with more advanced disease, confirm diagnosis, and recommend treatment • Have the ability to follow simple therapeutic protocols • Continuing education for all physicians, and as appropriate, for other members of the pediatric oncology team. Must attend at least one local/national/international conference or formal meeting devoted to pediatric oncology annually
LEVEL II POU • Level II POUs should be able to provide all the services of a Level I POU, and most/many of the services of a Level III POU • Level II POUs should work in close collaboration with a Level III POU locally or nationally • Level II POUs could be involved in the training of pediatric oncology specialists, but the main responsibility/direction of such training efforts would remain with the Level III units • Under the direction of the Level III POUs these units could participate in clinical trials and research.
Level III POU Center of Excellence • A Level III POU should be a special unit within a large general hospital, cancer center, pediatric department, or children’s hospital • Should be capable of treating all forms of pediatric cancers • Should have a minimum of 50 or more new diagnoses of pediatric cancer/year.
Certification or Needs Assessment Program • All Pediatric Oncology Units (irrespective of their level) should have a Needs Assessment visit by an identified body (national or international) • Once the level of the POU is established, it could be certified as such. • Units that lack specific components for certification could be given a report and time frame for improvement • This process of certification, though voluntary, could be used to obtain support and additional services from Ministries of Health, Governmental agencies or supporting NGO’S.
Establishment of a Pediatric Oncology Program and the Outcomes of Childhood ALL in a Resource-Poor Area • Retrospective cohort study in a pediatric hospital in Recife, Brazil • Assess the effect of a multi-disciplinary approach and protocol-based therapy on the event free survival of ALL • Scott Howard et al
Where does Ethiopia stand? • Between a Level I and Level III POU • Goal: • Improvement in services • Training of personnel • Upgrading of facilities • Use of a multi-disciplinary approach • Treatment protocols adapted to local conditions