Download
1 / 85
850 likes | 962 Views
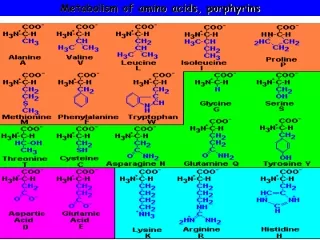
METABOLISM AND UTILIZATION OF AMINO ACIDS Rutgers School of Dental Medicine Spring, 2014. Carbon atoms ↓ Pyruvate, Acetyl - CoA , 2-OG , Acetoacetate , Suc - CoA. Amino nitrogen ↓ urea. AMINO ACIDS.

E N D
METABOLISM AND UTILIZATION OF AMINO ACIDS Rutgers School of Dental Medicine Spring, 2014
Carbon atoms ↓ Pyruvate, Acetyl-CoA,2-OG, Acetoacetate, Suc-CoA Amino nitrogen ↓ urea AMINO ACIDS Neurotransmitters (glutamate, aspartate, glycine) Anabolic pathways
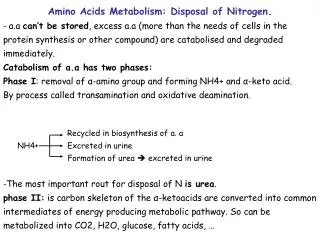
OUTLINE of PRESENTATION • Utilization of amino acid nitrogen • A) Transamination • B) Glutamate dehydrogenase reaction ammonia • C) Urea synthesis • 1) hyperammonemia, causes 2) HI/HA syndrome • Utilization of amino acid carbon • A) pyruvate gluconeogenesis
B) Acetyl-CoA fatty acids, cholesterol, steroids C) Acetoacetate “ketone bodies” D) Succinyl-CoA TCA cycle E) 2-oxoglutarate (α-KG) TCA cycle
III. Utilization of amino acids in anabolic pathways A) Creatine (arginine, glycine) B) Hormones Catecholamines(phenylalanine) Serotonin(tryptophan) Thyroid hormones(phenylalanine) C) Nitric oxide (NO) (arginine) D) S-adenosyl-L-methionine (SAM)(methionine) E) Cysteine (methionine, serine) F) Deoxyribothymidylic acid mono- phosphate (dTMP) (methionine re-synthesis)
“Inborn Errors” in Amino Acid Metabolism • A)Phenylketonuria (PKU)
I. Utilization of Amino-Acid Nitrogen A. Transamination1) Oxo- (keto-) acid co-substrate 2) Enzyme, Aminotransferase 3) Vitamin cofactor, Pyridoxalphos- phate NH2 O O O | | | | | | | R1CH– COH + R2 C– C– OH O O NH2 O | | | || | | R1– C – C– O H + R2–CH – C – OH
Oxoacid produces an Amino Acid: pyruvatealanine oxaloacetateaspartate 2-oxoglutarateglutamate* * leads to production of urea
2-OxoglutarateGlutamateGlutamateAmmonia AmmoniaUrea NH2 O | | | R– CH– C– O H + 2-OG O NH2 O | | | | | HO– C – CH2 – CH2 –CH – C– OH Glutamate NH3
B. GlutamateDehydrogenase Amino nitrogenAmmonia O NH2O | | | | | HO–C– CH2– CH2– CH - C – OH 2-oxoglutarate +NH3
C. Ureacycle First andRate-determiningStep CarbamoylphosphateSynthetaseNH3+ HCO3- + 2 ATP CARBAMOYL PHOSPHATE + Pi + 2 ADP
There are, in fact, two enzymes with this name. The urea cycle enzyme is Carbamoylphosphate synthetase I or CPS I
Step 1: Formation of carbamoylphosphate by CPS I, using nitrogenfrom ammonia(i.e., from amino acids), carbon from bicarbonate, and phosphatefrom ATP. O O │ │ │ │ H N - C - O - P - OH │ │ H OH
Step 2: Formation of citrulline Enzyme is OrnithineCarbamoyltransferase (aka ornithine transcarbamylase, OTC) Carbamoylphosphate + Ornithine Citrulline
Step 3: Formation of argininosuccinate by ArgininosuccinateSynthetase Citrulline + ASPARTATE+ ATP Argininosuccinate + AMP + PPi
Step 4: Cleavage of argininosuccinate to produce arginine and fumarate by ArgininosuccinateLyase Argininosuccinate Arginine+ Fumarate
Step 5: Formation of urea and regeneration of ornithine by Arginase Arginine + H2O UREA+ Ornithine
CARBAMOYL PHOSPHATE + UREA Ornithine Citrulline Arginine + UREA CYCLE Aspartate Fumarate Argininosuccinate
REGULATION of the UREA CYCLE acutely: N-acetylglutamate (NAG) is an allosteric effector that upregulates CPS I. NAG is synthesized from acetyl-CoA and glutamate. via gene expression:Hepatic nuclearfactors (HNFs) are required for transcription of the CPS I gene hence, tissuespecificity!
N-Acetylglutamate (NAG), from glutamate and acetyl-CoAvia NAG synthase
HYPERAMMONEMIA (Ammonia Toxicity) Hyperammonemia represents a neonatal emergency. It is manifested by high toxicity to the central nervous system accompanied by developmental delay. Causes: defects in urea cycle enzymes, organic acidemias, congenital hyperinsulinism with hyperammonemia.
Observed Pathology: brain edema, astrocyte dysfunction Clinical Manifestations: anorexia, irritability, somnolence, disorientation, brain edema, coma, death
Due to its sensitivity with respect to ammonia, the brain’s astrocytes exhibit very high leveels of glutamine synthetase(GS) activity. Glutamate + Ammonia + ATP →→→ Glutamine + ADP + Pi
Detoxification of ammonia in the liver. Brain also uses the formation of glutamine by glutamine synthetase (GS).
When the urea cycle fails to function normally, blood concentrations of NH3 rise. Since NH3 passes the blood/brain barrier (BBB), concentrations of NH3 in the brain rise to levels that become toxic.
In the brain, excessive NH3 can lead to increased intracellular calcium (Ca2+) levels that, in turn, lead to an increase in reactive oxygen (or nitrogen) species. These can produce mitochondrial (astrocyte) dysfunction such as that associated with ammonia neurotoxicity.
GENERAL MANAGEMENT Alternative pathway therapy: 1) Sodium benzoatehippuric acid 2) Sodium phenylacetateorsodium phenylbutyratephenylacetylglutamine
In the brain, glycine synthase converts ammonia into the glycinenitrogen, i.e., NH3 + CO2 + methylene (-CH2-) of 5,10-methylene tetra- hydrofolate (THF) + NADH glycine synthase NH2 І CH2 – C O O H + NAD+ + H2O
Then, glycine + benzoate benzoylglycine (akahippuric acid), which is then excreted in the urine.
Alternatively,, conversion of ammonia nitrogen into glutamine nitrogens: 1NH3+ 2-oxoglutarate + NADH glutamate + NAD+ + H2O followed by 1 NH3+ glutamate + ATP Glutamine (twonitrogens) + ADP + Pi
Then, glutamine + phenylacetate or phenyl- butyrate phenylacetylglutamine, which is then excreted in the urine.
More recently, particularly in neonates exhibiting hyperammon-emia, N-carbamoylglutamate, i.e., carglumic acid, is used along with conventional therapy. Carglumic acid is reported to act directly on CPS I to enhance flow through the urea cycle.
Action of N-carbamoylglutamate (carglumic acid) on the Urea Cycle PA – propionic acidemia; MMA – methylmalonicacidemia
However, in the case of the extensively studied hyperinsulinismwithhyperammonemia syndrome (HI/HA or HH syndrome), this analog of N-acetylglutamate is not the drug of choice because HI/HA syndrome is caused by a mutation in the glutamate dehydrogenase gene.
The mutation is a so-called “gain-of-function” mutation which produces GDH that is no longer negatively controlled (down regulated) as it should be. Thus, in HI/HA synsdrome patients, there is a “super-active” GDH.
Glutamate dehydrogenase (GDH) is key not only in carbohydrate metabolism but also in amino acid metabolism. GDH converts glutamate into ammonia (a substrate in RDS of urea cycle) and 2-OG (key component of the TCA cycle). Further, excess GDH activity means lessNAG, needed to activate CPSI.
Patients (most frequently children) with HI/HA syndrome often present with increased pancreatic β-cell responsiveness to protein intake, leading to hypersecretion of insulin accompanied by mildly increased levels of blood ammonia.
Signaling involved is as follows: 1) Protein intake means intake of (essential) amino acids, including branched-chain amino acids (BCAAs). 2) Utilization of BCAAs begins with their transamination (BCAT), which requires 2-OG as the co-substrate. Hence, glutamate is generated.
3) Normally, this glutamate undergoes transamination preferentiallywith pyruvate. Thus, alanine would be formed. In the HI/HA syndrome patient, a super-active GDH means that this glutamate becomes a substrate for GDH. NH3 and 2-OG are generated.
4) Excessive 2-OG promotes excessiveTCA cycle activity that generates increased ATP. This leads to events that ultimately result in increasedinsulinsecretion from the pancreatic β-cell, as illustrated on the next slide.
Secretion of Insulin by the Pancreatic β Cell: 1) Glucose enters the pancreatic cell, undergoes glycolysis, TCA cycle, ATP produced. 2) Increased ATP closes K+ (SUR, KIR) channels, cell undergoes depolarization. 3) Ca2+ enters the cell and acts on Insulin Granules. 4) Insulin is secreted via exocytosis.
Hence, the patient with HI/HA syndrome exhibits hypoglycemia, resulting from increased protein-induced insulin secretion. This is accompanied by a mild hyperammonemia resulting from the increased ammonia that was also produced by the “super active” GDH.
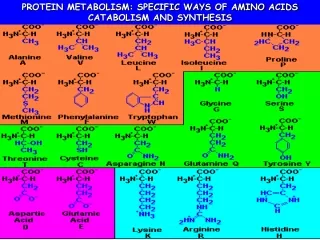
II. Utilization of Amino-acid Carbon Carbon atoms of amino acids are cataboliz-ed by being incorporated into specific well-known biochemical intermediates, i.e., 1) pyruvate 2)acetyl-CoA 3)acetoacetate 4)succinyl-CoA 5)2-oxoglutarate
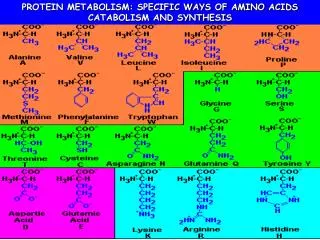
1. Carbon atoms from amino acids below become those of pyruvate. Glycine Serine Cysteine Aspartate Alanine Tryptophan Pyruvate
Significance: pyruvate Glucose (via gluconeogenesis) Acetyl-CoA(via Pyruvate Dehydrogenase Complex)
2. Carbon atoms of amino acids below become those of acetyl-CoA. Leucine Isoleucine Tryptophan Lysine Acetyl-CoA
Significance: Acetyl-CoA Cholesterol and Steroids (via de novo cholesterol synthesis TCA Cycle (substrate in the RDS) Palmitic Acid (substrate in de novo FA synthesis)
3. Carbon atoms of amino acids below become those of acetoacetate. Phenylalanine Tyrosine Acetoacetate
Significance: Acetoacetate is one of the “ketonebodies”and the source of the other two. Acetoacetate loss of CO2 reduction (ketone) Acetone 3-Hydroxybutyrate
“Ketone bodies” have a critical function since they are utilized (as an energy source) by the brain during carbohydrate deprivation. However, their over productionin the diabetic patient leads to metabolic acidosis.