Using Pre-Mixed Insulin Case Study
Using Pre-Mixed Insulin Case Study. Lucia M. Novak, MSN, ANP-BC, BC-ADM The Diabetes Institute Walter Reed Army Medical Center, Washington, DC Adjunct Assistant Professor, Graduate School of Nursing, Uniformed Services University of the Health Sciences, Bethesda, MD.

Using Pre-Mixed Insulin Case Study
E N D
Presentation Transcript
Using Pre-Mixed InsulinCase Study Lucia M. Novak, MSN, ANP-BC, BC-ADM The Diabetes Institute Walter Reed Army Medical Center, Washington, DC Adjunct Assistant Professor, Graduate School of Nursing, Uniformed Services University of the Health Sciences, Bethesda, MD
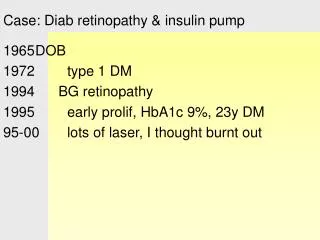
Premixed Insulin Case Study~John~ 72 yo African American man Presents with complaint of frequent episodes of weakness and “nervousness” in the evening His wife died 1 year ago and he now lives alone His schedule is erratic, some days he wakes up at 6AM, other days he sleeps until 10AM because he has been up late watching TV. On the days he wakes up late, will have late breakfast, will skip lunch and eat an early dinner. Most of his meals are “frozen TV dinners.” He will have a snack when he gets home because he feels nervous His exercise consists of an evening walk he likes to take after he eats dinner
Pertinent History • Past Medical History: • Type 2 Diabetes Mellitus (15 years) • Coronary Artery Disease (MIx1 15 years ago, 2vCABG) • Hypertension (20 years) • Dyslipidemia (20 years) • Benign Prostate Hyperplasia (10 yrs) • Social History: • Widower, no children • Active in his retirement community • Former smoker, quit 15 years ago • Occasional beer
DM Management • Current: (2 yrs) • PreMixed 70/30 Human Insulin (NPH/REG) • 18 units “in the morning” • 14 units “in the evening” • Previously • Bed time NPH and daytime glipizide and metformin • Stopped because not good control and switched to above • Pt. refuses to take more than 2 shots a day
Other medications • ECASA 325 mg • Statin for cholesterol • CCB for blood pressure • ACE-I for blood pressure • BB for blood pressure • Diuretic for blood pressure • A1-blocker for BPH • OTC • Acetaminophen as needed
24 hour diet recall • Breakfast 7am – 10:30 AM • Coffee, bowl of instant oatmeal, canned fruit • Lunch: only if breakfast before 8AM • Can of soup, ½ gr cheese sandwich, diet soda • Dinner: between 4:00 and 7:30 pm • TV dinner: salsbury steak, mashed potatoes, green beans • Snacks: most often in evening, a candy bar or a sugar-free pudding with a cookie
Review of Systems • General: • Feels fine, denies any complaints other than late day nervousness • Eyes: • Last retinal exam 3 months ago, +mild-mod NPDR OU • CV: • Denies CP, SOB, DOE, postural dizziness • Neuro: • intermittent tingling and burning to both feet • GU: • nocturia 1-2x nightly
Latest labs values (1 week ago) • A1C: 8.5% (range 7.5 – 8.7% for last 2 years) • Fasting Glucose: 163 mg/dL • Scr: 1.7 mg/dL • GFR: 45 mL/min • AST: 32 U/L • ALT: 24 U/L • Microalb/creatinine: 76.2 mg/g CRT • LDL-C: 66 mg/dL • TG: 132 mg/dL
PE • Vitals: • B/P: 124/62, HR: 98 reg • Ht: 67” Wt: 180 lbs BMI: 28 kg/m² • General: • Well-nourished, well-developed • African American man, A&Ox4, NAD
What are YOUR concerns? • Hypoglycemia • Elderly • Long-standing DM with micro- and macrovascular complications: • Retinopathy, nephropathy, neuropathy • +Cardiac disease • Lives ALONE • Very active • Considerations: • Pt refuses > 2 “shots” a day • Erratic sleep/wake schedule • Erratic meal times • Enjoys evening walk
s.c. injection Mixed Insulin Replacement Therapy Normal Insulin Secretion at Meal Time Analog Mix PreMix 70/30 (NPH/REG) Change in Serum insulin Time (hours) 75/25 Humalog Mix 70/30 Novolog Mix
Treatment Strategies • Easier to change medications than to change habits • Analog Mix insulin can be dosed once, twice or three times a day • Available in Prefilled Pens • No need to time insulin far in advance of meal • When food “in front of you” • While eating • As late as 15 minutes after eating • Want him to continue to exercise!! • What about dinner dose? • Snack? • Appropriate A1C goal: • Given his age, duration of DM, +complications, +Cardiac Hx • ACCORD, ADVANCE, VADT • Pt. education: • Treatment of hypoglycemia
Treatment of Hypoglycemia“Rule of 15” Check BG when hypoglycemia is suspected (<70) Treat with fast-acting source of carbohydrate: (15 grams) 4 glucose tabs, or 3 packets of sugar 1 cup (8 oz) SKIM milk 1/2 cup (4 oz) fruit juice or non-diet soda 8-10 fruit-flavored lifesavers or 3 peppermint stars Wait 15 minutes!!! Recheck blood sugar (must be >70) Retreat if necessary. Activate EMS if BG <70 after 3 treatments Teach significant others to use glucagon should pt become unconscious Eat meal or snack: protein/CHO Adjust treatment plan if frequent hypoglycemia
Preventing Hypoglycemic Emergencies Test BG OFTEN >4 times daily, record, analyze Test BG immediately when feeling hypoglycemic Immediately and precisely treat hypoglycemia Identify the earliest signs of hypoglycemia and pay attention to them Test BG immediately before driving and do not drive if BG <110 Cognitive recovery 45-75 min after BG < 50 Carry a rapidly absorbed glucose source Wear a medical ID Glucagon kit for emergencies