Download
1 / 11
110 likes | 312 Views
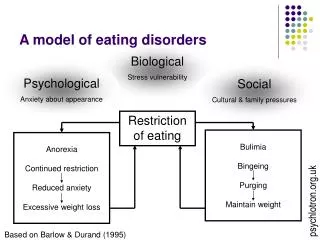
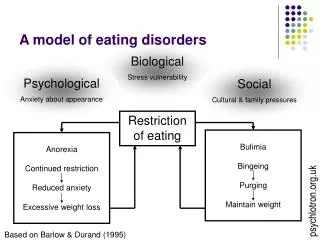
Biological Stress vulnerability. Psychological Anxiety about appearance. Social Cultural & family pressures. A model of eating disorders. Restriction of eating. Bulimia Bingeing Purging Maintain weight. Anorexia Continued restriction Reduced anxiety Excessive weight loss.

E N D
Biological Stress vulnerability Psychological Anxiety about appearance Social Cultural & family pressures A model of eating disorders Restriction of eating Bulimia Bingeing Purging Maintain weight Anorexia Continued restriction Reduced anxiety Excessive weight loss psychlotron.org.uk Based on Barlow & Durand (1995)
Treatments for EDs • Behaviour therapy • Cognitive behaviour therapy • Weight restoration (anorexia only) psychlotron.org.uk
CBT • Treatment based around: • Identifying dysfunctional thinking processes that cause & maintain disordered eating • Use of behavioural exercises to test and modify maladaptive beliefs psychlotron.org.uk
CBT with bulimia nervosa • Four stages (Fairburn, 1985): • Education about effects of bingeing, purging, dieting • Modified eating patterns – small meals 5-6 times a day • Altering dysfunctional attitudes about food, eating & the body • Teaching coping strategies to avoid bingeing & purging psychlotron.org.uk
CBT with bulimia nervosa • Fairburn et al (1993); comparison of three treatments: • CBT (all four parts) • BT (just the eating habits part) • IPT (interpersonal therapy) • Outcome measures: cessation of bingeing/purging; attitudes to body/eating psychlotron.org.uk
IPT CBT Cessation rate 0 20 40 60 BT Start End 4mo 8mo 12Mo CBT with bulimia nervosa psychlotron.org.uk
CBT with bulimia nervosa • CBT works fast & is more effective than BT • Not a panacea – only 36% had no symptoms at 1 year follow-up • Early treatment gains may be lost; IPT more effective long term • Drugs may boost effectiveness (Agras et al, 1992) psychlotron.org.uk
CBT with anorexia nervosa • Anorexia involves several cognitive distortions: • Irrational beliefs about food & weight gain • Inaccurate perception of body • CBT aims to change these thinking patterns, which are assumed to maintain anorexia behaviour psychlotron.org.uk
CBT with anorexia nervosa • Treatment goals (Yager, 1994): • Educate & inform about anorexia • Identify & focus on unhelpful thoughts & beliefs • Replace these with more adaptive ways of thinking • Identify problems & develop problem solving strategies psychlotron.org.uk
CBT with anorexia nervosa • Improved body image, eating habits at 7-year follow up (24 patients; Yager, 1994) • Can be effective in helping maintain weight but many continue to have distorted body image (Davison & Neale, 1994) psychlotron.org.uk
CBT with anorexia nervosa • Highly structured treatments (BT, CBT) most effective during initial treatment (<1 year) • In longer term, patients may benefit more from psychotherapy/IP/family therapy • Addressing underlying problems? Compare bulimia treatment data. psychlotron.org.uk