Download
1 / 91
910 likes | 926 Views
This event showcases the second wave of the Police Healthcare TransferWave programme, highlighting the need for better healthcare for offenders and the benefits of integrating healthcare across the criminal justice system. Key topics include mental health, substance misuse, public health, and liaison and diversion schemes.

E N D
Police Healthcare TransferWave 2 Launch 27th March 2012
Direction Setting Richard Bradshaw Director of Offender Health (Department of Health / National Offender Management Service
The case for change 40-70% of police detainees are under the influence of alcohol, peaking during evenings and weekends 90% of prisoners have a diagnosed mental health problem, and over a third of children and young people in custody. Some older prisoners have a physical health status of 10 years older than their contemporaries on the outside 40- 50% of prisoners are drug dependent. 24% inject. Over a third of children and young people accessing substance misuse services are from the youth justice system.
NHS Reform Liberating the NHS: Bold reforms to the NHS as set out in response to the NHS Future Forum (DH, 2011). Public Health England Healthy Lives, Healthy People, a strategy for Public Health in England (DH, 2010). Mental Health No Health without Mental Health, a cross-Government mental health outcomes strategy for all people of all ages (DH, 2011). Breaking the Cycle: Effective Punishment, Rehabilitation and Sentencing of offenders (Ministry of Justice, 2010). Criminal Justice Green Paper Reducing demand, restricting supply, building recovery: supporting people to live a drug-free life (Home Office, 2010). Drugs Social Care A vision for adult social care: Capable communities and active citizens (DH, 2010) The policy context…
Andrew Lansley, Secretary of State for Health “We need to do better…true justice for the most vulnerable is about pulling people into treatment, not pushing them away from the support they need. People should get the same quality of services in prison as they do in the community…we have to do more in early intervention, to support children and young people before they reach crisis point…we need diversion services to be a cornerstone of better care and support for offenders with mental health problems.” Speaking at Care not Custody Campaign Event, March 2011
Building on Bradley • Continued commitment to meeting the health needs of offenders – via a co-ordinated approach. • Changes to commissioning arrangements – the NHS Commissioning Board. • Work across Government will focus on following priorities for health and criminal justice: • Transition • Liaison and Diversion • Police and Health Partnerships • Drugs and Alcohol • Public Health
Liaison and Diversion Government commitment to make liaison and diversion schemes nationally available by 2014, subject to business case approval £19.4m investment for 2012/13 Develop process in police custody 101 members of new network comprising: 54 adult sites, of which 20 pathfinders will support evaluation study 2 new diversion schemes 31 youth justice sites (including six existing pilots) 10 police transfer early adopter sites 4 Community Safety Partnership / Drug Action Team sites
Police and Health Partnerships Current model supports short-term healthcare of a detainee or victim and to enable a criminal investigation to proceed. Only stage in the adult criminal justice pathway where healthcare is not commissioned by the NHS. Has wide-spread support (including ACPO) due to the clear benefits of integrating the healthcare pathway across the criminal justice system and was a key Bradley recommendation.
Police and Health Partnerships Voluntary approach agreed with Home Office whereby individual Police Forces opt into commissioning partnerships with local NHS. Supports Coalition’s localism agenda and introduction of Police and Crime Commissioners next year. Three waves of new partnerships until 2014. Responsibility then expected to formally transfer to NHS from next Spending Review. Ministerial approval received.
Police and Health Partnerships post 2015 NHS Commissioners managing responsibility for police custody and diversion. Joined up offender health economies and pathways. One conversation in custody producing further efficiencies.
Commissioning Police Healthcare Transfers – Launch of 2nd Wave Event Sally Richards – Reducing Reoffending Unit, Home Office
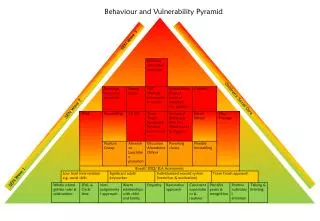
To reduce crime there is a need to tackle the underlying physical and mental health issues that can contribute to individuals offending Alcohol is a factor in an estimated 44% of violent crime Some evidence that A&E data sharing and targeted interventions can reduce alcohol related disorder by around ¼ Drug users are responsible for between 1/3 and 1/2 of acquisitive crime Treatment can cut the level of crime they commit by about half Over 90% of prisoners have one or more psychiatric disorders (including alcohol and drug dependence) Liaison and diversion schemes aim to increase the standard of care and support and link people to treatment and appropriate activities across the CJS and outside, where appropriate There is a clear link between certain health needs and offending behaviour Young people in the youth justice system have significantly higher levels of health needs than the general population and differing health needs to adult offenders Significant proportion of crime is committed by young and adult offenders who have substance misuse and/or mental health problems. Learning difficulties and disabilities also relevant factors There have been significant gains in the integrated delivery of health and criminal justice interventions and treatment 13
Building on what works: Multi Agency Working The Drug Interventions Programme showed how multi agency working is key to tackling health and crime reduction outcomes • OVERVIEW • DIP plugs the gaps between CJS and community and manages individuals into recovery journeys. • DIP repeatedly grips people as early as possible and at every opportunity. • It works alongside the CJS, complementing and not duplicating processes. Police Local Community The same should apply for wider health needs Courts Probation DIP now being embedded in local Integrated Offender Management approaches with the police as key partners Prison CJS Main DIP points of contact with drug using offenders 1
Changes to the local landscape: Police Reform • From November 2012 directly elected Police and Crime Commissioners (PCCs) will ensure local police force is held to account by the community it serves. • As well as their core policing role, PCCs will have a remit to cut crime and will have commissioning powers and funding to enable them to do this. • Part of a package of Reforms: • Establishment of the National Crime Agency • New Police Professional Body • Winsor review, IT and procurement changes Home Secretary: “all of these reforms are fundamentally about increasing the police’s ability to fight crime” • Collective local leadership on crime, justice and community safety will be the key to cutting crime and improving outcomes for local people. • Reducing crime requires a strong health input on issues such as drug and alcohol dependence and mental health. By co-commissioning services effectively with Health agencies, all partners could work with those individuals that cause the most harm, and the most cost, to local communities. 15
Home Office Ministerial Support Significant growing interest in mental health issues across the CJS Localism - ensuring local arrangements meet local needs Encouraging local partnership working between Health and CJS agencies Home Office are partners in the Police Healthcare Oversight Programme – we want you to show us how this will work 16
Police Healthcare Commissioning TransferWave 2 Adopters National Launch Tuesday 27th March 2012 David Whatton Chief Constable ACPO lead for Adult Sex Offences
History What we have now What is covered Why we have them Keep detainees safe Victim care/evidence recovery arrest offenders Healthcare in the Police
Victims of Sexual Assault Programme - Positive & Welcome Opportunities First Phase Second Wave Why? Early Adopter Programme
Funding: - complicated and varied (PCT’s/LA/PA) - long term future – uncertainty Forensic Practitioners: - not enough - training/experience Children & Young People: - paediatricians - services provided/safeguarding issues Minimum Standards - checked, how? - common care pathways for SARC services Complex - Current Issues
Tip of the ice berg • What we know/what we don’t know • How do we uncover the rest of this • No one agency will achieve this alone • Need public confidence • Develop capacity to grow with demand
SARC – Fundamental to building public confidence • Who commissions these services • Who funds these • Who governs these services Different in each area !!
“I’ve seen the statistics for prosecution of this sort of thing so what would be the point? It would only cause myself more trouble.” Hidden Marks: NUS study of women students experiences 18 March 2010 “I went to my GP and he wouldn’t believe me. He even wrote ‘raped’ in inverted commas on my doctor’s note. What if I needed my medical records in court?” Sara Payne Review 2009 Do victims have confidence in public authorities?
EAP 2nd WaveSexual Assault Services – Department of Health Amy Nicholas Violence and Social Exclusion Team
Policy objectives • Improve the quality of services to victims of rape and sexual assault • Improve the experience of victims of rape and sexual assault • Deliver equity of access to resources across England • Ensure forensic competence of practitioners through improved clinical governance, peer review and accredited training • Optimise the potential to raise prosecution rates in cases of rape and sexual assault
Policy now “ We have decided that subject to resolving some further points of detail, responsibility for sexual assault services, including SARCs, at least in the short to medium term, should rest with the NHS Commissioning Board.” Public Health in Local Government Factsheets http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_131889
The best of both worlds Local National • Capability • Address equity and health inequalities on a national scale • Comply with NHS standards • Understands clinical service commissioning • Achieve economies of scale- both commissioning and service provision • Connectivity to NHS workforce development • Develop referral pathways into further healthcare • Partnerships: • Police Constabularies • police crime commissioners • Community safety partnerships • open sexual health services • wider public health role of local authorities
Where we are coming from • 2002 HMCPSI/HMC Thematic Inspection of Rape, 2002; subsequent HMCPSI/HMIC joint review, Without Consent, 2005 • 2009Improving Health, Supporting Justice • 2009 Together We Can Tackle Violence against Women and Girls • 2009 Revised National Service Guide: A Resource for Developing Sexual Assault Referral Centres. • 2010 Responding to Violence against Women and Children – the Role of the NHS • 2010 Independent Review of How Rape Complaints are Handled by Public Authorities in England and Wales • 2010 Call to End Violence against Women and Girls: The Strategy • 2010 Improving Services for women and child victims of Violence • 2011 Call to End Violence against Women and Girls: Action Plan • 2011 The Government’s Response to the Stern Review • 2011 Feasibility of Transferring Budget and commissioning Responsibility for Forensic Sexual offences Examination Work from the Police to the NHS
Key influences on way forward – Health and care • Healthy Lives, Healthy People • Healthy Lives, Healthy People: Consultation on the Funding and Commisssioning Routes for Public Health • Healthy Lives, Healthy People: Update and Way Forward • Healthy Lives, Healthy People: Public Health in Local Government - factsheets Public Health Reforms NHS Reforms • “In the consultation document we said that it would make sense for the NHS commissioning Board to have responsibility for health services for those in prison or custody. We received no objections to this and will proceed on this basis.” • Liberating the NHS: Commissioning for Patients • Liberating the NHS: Legislative Framework and Next Steps
Key influence - Crime and violence Crime and Violence “The ambition of this Government is to end violence against women and girls.” Localism
The new public health system • Accountability to SoS • PHE accountable for: • protecting health • coordinating improvement against PH outcomes • assuring NHS CB meet 7A contract • assuring LA meet requirements of SoS (mandatory services incl core offer to NHS) • publish outcomes • NHS CB accountable for: • Mandate • Section 7A PH services • PHE and NHS CB • PHE to assure section 7A and PH mandate delivery • NHS CB to assure delivery PH advice and core offer • PHE and LA • Delivery of mandatory services, grant conditions, reporting PH outcomes for HP • Local Accountability • LA and HWBB accountable to local people • PHE/CCG+NHS CB health protection plans to be assured by DPH • HWBB oversight of need and strategy Secretary of State 1 1 2 3 PHE NHS CB 2 4 3 LA PHE (local) 6 6 CCG/NHS CB 7 7 7 4 HWBB 5 5 6 Local people and communities 7
Low volume of cases 28/100,000 resident population Inadequate commissioning standards and capability Variable local partnerships Service quality below acceptable standards Inequitable resource provision across care pathways Inconsistent provision of forensic medical response No strategic development of clinical workforce Poor public knowledge about sexual assault services, standards, when and how to access them The problem - University of Birmingham Feasibility Study
Wide variation in provision of forensic examination services
NORTH (NW, NE, Y&H) 1. Lancashire 2. Greater Manchester & Cheshire Merseyside 4. Cleveland 5. Durham Northumbria 7. Humberside 8. South Yorkshire (Cumbria, N.Yorkshire, W.Yorkshire) SOUTH (S.West, S.Central, S.East Coast) 1. Avon & Somerset 2. Devon & Cornwall – Plymouth Devon & Cornwall – Truro Dorset Gloucestershire Wiltshire Hampshire Kent Surrey Sussex Thames Valley MIDLANDS (WM, EM, E of England) Staffordshire 2. Derbyshire 3. Leicestershire 4. Lincolnshire 5. Nottinghamshire 6. Northamptonshire 7. Cambridgeshire 8. Essex 9. Norfolk 10. Suffolk (Warwickshire, W.Mids,W.Mercia, Bedfordshire,Hertfordshire) LONDON Camberwell Paddington Whitechapel SARCs now
The transition Opportunities Risks Early Adopter Programme • Loss of commissioning • capability • Stagnating PCT investment • De-investment by Police • Loss of focus on children’s issues • PCCs • Early Adopter Programme • NHS CB share of public • health ring-fence budget • PCCs
Governance of Programme and expectation of Partnership Andy Hunt
Strategic Benefits Transfer risk Safer Detention Health Inflation Reduce crime Health Equality Prevention
Governance of Programme Overall programme answerable to Health and CJ Transition Board Part of Diversion Programme Overseen by Police Healthcare Oversight Board with key strategic membership Stakeholder Group Early Adopter Forum and Second Wave Forum to share good practice and solve problems
Partnership Boards 10 police early adopter sites selected for 2011/12. 20 for 2012/13 National Police managers appointed to support activity Funding provided to support transition for 2 years Desire to include sexual assault referral provision
Scope for the parternship Form shadow partnership with local NHS commissioners, with appropriate Governance arrangements Full audit of current healthcare spend to support future evaluation activity Full health needs assessment via NHS Commissioner to define future provision Develop future commissioning models to inform the diversion work programme
Scope for parternship Understand IT requirement Set police user scope Evaluate full cost of new service ( by procurement or otherwise) Develop Care pathways for s 136, drunk and incapable, packers and swallowers Sign statement of readiness Develop diversion as it is mainstreamed Transfer responsibility
National Support • Programme manager • Experience of EA partnerships • Utilisation of existing templates for good practice IT Memorandum of Information
CommunicationsNHS Networks New communications vehicle to facilitate an online community – NHS Networks. www.networks.nhs.uk/nhs-networks/health-and-criminal-justice-liaison-and-diversion