Download
1 / 44
460 likes | 702 Views
Current Diagnosis and Mechanisms of Glucose Dysregulation. Dr. Josephine Carlos-Raboca Chief, Section of Endocrinology, Diabetes & Metabolism Makati Medical Center Immediate Past President, PSEM. Outline. Overview of glucose regulation Stages of Dysglycemia (glucose dysregulation)

E N D
Current Diagnosis and Mechanisms of Glucose Dysregulation Dr. Josephine Carlos-Raboca Chief, Section of Endocrinology, Diabetes & Metabolism Makati Medical Center Immediate Past President, PSEM
Outline • Overview of glucose regulation • Stages of Dysglycemia (glucose dysregulation) • Current Diagnostic Criteria for dysglycemia • Mechanisms of Glucose Dysregulation • Summary
Glucose Metabolism Tightly regulated to maintain adequate plasma levels Major hormones • insulin • glucagon • incretins Major organs • islet cells of pancreas • insulin sensitive organs: liver, muscle, fat • intestines • Kidneys Modulator • Endocannabinoid System
Islet as an Organ: Role of Pancreatic Islets in Normal Glucose Homeostasis
Islet of Langerhans ~ 3,000 cells 75% Beta cells 25% non-Beta cells 200 µm Micrograph: Lelio Orci, Geneva
Beta and Alpha Cells in the Pancreas of Normal Individuals 1. Cabrera O et al. PNAS. 2006;103:2334–2339. 2. Cleaver O et al. In: Joslin’s Diabetes Mellitus. Lippincott Williams & Wilkins; 2005:21–39.
Insulin Production • Primary regulators for insulin biosynthesis • glucose • glucagon • incretins- GLP-1, GIP • Inhibits insulin biosynthesis • catecholamine • somatostatin
Glucagon • Main regulator- glucose amino acids • incretins • Insulin • fatty acids • ketones
Insulin and Glucagon Regulate Normal Glucose Homeostasis (–) (–) (+) (–) (+) Liver Glucagon (Alpha cell) Pancreas (+) Insulin (Beta cell) Glucose uptake Glucose output Blood glucose Muscle and adipose tissue Porte D Jr et al. Clin Invest Med. 1995;18:247–254. Adapted from Kahn CR, Saltiel AR. Joslin’s Diabetes Mellitus. 14th ed. Lippincott Williams & Wilkins; 2005:145–168.
GUT and GUT Hormones • Na ATP channels – absorption of glucose • Incretins
Incretins Regulate Glucose Homeostasis Through Effects on Islet-Cell Function Ingestion of food Insulinin glucose-dependent way from β cells(GLP-1 and GIP) Increased peripheral glucose uptake Release of incretin gut hormones GI tract Pancreas INSULIN Bloodglucose control Bloodglucose control β cells α cells Active GLP-1 and GIP ↓GLUCAGON Decreasedhepatic glucose output Glucagon in glucose- dependent way from αcells (GLP-1) InactiveGLP-1 (9-36) and GIP (3-42) Adapted from Brubaker PL, Drucker DJ. Endocrinology. 2004;145:2653-2659;Zander M et al. Lancet. 2002;359:824-830; Ahrén B. Curr Diab Rep. 2003;3:365-372; Buse JB et al. In Larsen PR et al, eds.: Williams Textbook of Endocrinology. 10th ed. Philadelphia, PA: Saunders; 2003:1427-1483.
The endocannabinoid system is a modulatory system • Endocannabinoids: • Synthesized on demand from lipid precursors in postsynaptic cell • CB1 receptors: • Play a key role in energy balance and lipid and glucose metabolism Di Marzo V et al, 2005; Di Marzo V et al, 1998; Wilson R et al, 2002
Central and peripheral targets of the endocannabinoid system Brain Peripheral tissues Adipose Liver Muscle tissue GI tract Hypothalamus: Nucleus accumbens: ^ ^ hunger motivation to eat Insulin resistance ^ HDL-cholesterol Triglycerides ^ Increased food intake Glucose uptake Increased fat storage Adiponectin HDL: high-density lipoprotein Bensaid M et al, 2003; Pagotto U et al, 2005; Osei-Hyiaman D et al, 2005; Di Marzo V et al, 2005; Liu YL et al, 2005
Regulation of glucose Homeostasis • Na dependent transporters in proximal tubules of kidneys cotransport glucose with sodium maintained by Na+/K+-ATPase ion pump
Glucose homeostasis • Is a balance of glucose appearance and disappearance • Glucose appearance: endogenous glucose production (liver, muscle and kidneys) exogenous sources (GIT) affected by feeding signals • Glucose disappearance peripheral uptake from liver, muscle and fat
Current Diagnosis of Prediabetes and Diabetes
Definition of Diabetes • A metabolic dysregulation • Hallmark: hyperglycemia • Basic defects: • Islet cell dysfunction • Insulin insensitivity • Impaired action of insulin on target tissues
Definition of Diabetes • Chronic hyperglycaemia associated with long-term damage to: • Eyes • Kidneys • Nerves • Heart and blood vessels
Hyperglycemia Stages Diabetes Mellitus Impaired Glucose Tolerance or Impaired Fasting Glucose (Pre-Diabetes) Normal Glucose Regulation Type Not insulin requiring Insulin requiring for control Insulin requiring for survival Type 1 * Type 2 Other Specific Type * Gestational Diabetes **
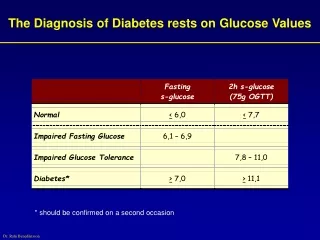
Diagnostic Criteria For DM American Diabetes Association 2003 ADA, Diabetes Care 2009
Hba1c • Integrated summary of circadian blood glucose in the preceding 6-8 weeks • Not used as diagnostic test for diabetes • Lack of standardized analytical method and therefore lack of a uniform non diabetic reference level between laboratories • Insensitive in the low range • Normal aic cannot exclude diabetes or IGT
Issues on current diagnostic cut off • 3 studies on which FPG of 7.0 cutoff was based for diagnosis of diabetes used direct ophthalmoscopic examination and one retinal photograph • Diabetes Prevention Program showed substantial prevalence of retinopathy below FPG of 7.0 • Cardiovascular complications occur at lower glucose levels • Definition and classification of diabetes and pre states should be based on the level of subsequent risk of cardiovascular complications class 1 level B ESC,EASD 2007
Relation between FPG and retinopathy BMES AusDiab MESA • FPG 5.3 6.5 5.9 • (Mean) • Number 364 210 959 • (%) with (11.5) (9.3) (15.8) Retinopathy • Lancet 2008
Blue Mountains Eye Study (5-year incident retinopathy) Any retinopathy Percentage Fasting plasma glucose (mmol/L) Relation between baseline FPG and incident retinopathy, BMES
Recommendation • Current diagnostic criteria remain the best tools for now.
Mechanisms of Glucose Dysregulation and Development of Type 2 Diabetes
Genetics • 39% of patients with type 2 diabetes have at least one parent with the disease • Among monozyzgotic twin pairs with one affected twin, approximately 90% of unaffected twins eventually develop the disease • First degree relative of patients with type 2 diabetes frequently have impaired nonoxidative glucose metabolism long before they develop type 2 diabetes • Ethnic predilection
Environment • Low birth weight • Gestational diabetes • Prematurity • Sedentary lifestyle • High fat diet
Physiologic & Molecular basis of Diabetes • Physiologic islet cell dysfunction insulin resistance • Molecular insulin receptor Insulin signal transduction
Beta-Cell Function Is Abnormal in Type 2 Diabetes • A range of functional abnormalities is present • Abnormal oscillatory insulin release • Increased proinsulin levels • Abnormal insulin response • Progressive loss of beta-cell functional mass Adapted from Buchanan TA Clin Ther 2003;25(suppl B):B32–B46; Polonsky KS et al N Engl J Med 1988;318:1231–1239; Quddusi S et al Diabetes Care 2003;26:791–798; Porte D Jr, Kahn SE Diabetes 2001;50(suppl 1):S160–S163.
First-Phase Insulin Response to IV Glucose Is Lost in Type 2 Diabetes Type 2 Diabetes Normal 120 120 100 100 80 80 Plasma insulin (µU/mL) Plasma insulin (µU/mL) 60 60 40 40 20 20 0 0 –30 0 30 60 90 120 –30 0 30 60 90 120 Time (min) Time (min) n=9 normal; n=9 type 2 diabetes. Adapted from Pfeifer MA et al. Am J Med. 1981;70:579–588.
Normal Compensation More islets Larger islets More beta cells/islet Larger beta cells Nondiabetic Obesity Decompensation Fewer islets Fewer beta cells/islet Amyloidosis Type 2 diabetes Fewer Pancreatic Islets in Type 2 Diabetes Adapted from Rhodes CJ. Science. 2005;307:380–384.
Increased Beta-Cell Apoptosis Occurs in Type 2 Diabetes * *p<0.05. Islet cell death was assessed by an ELISA method, which evaluates the cytoplasmic histone-associated DNA fragments. After incubation absorbance of samples was read spectrophotometrically. Data obtained from pancreatic islets isolated from 6 T2DM organ donors and 10 nondiabetic cadaveric organ donors. Adapted from Marchetti P et al. J Clin Endocrinol Metab. 2004;89:5535–5541.
Amylin • Amylin co-secreted with insulin • Low amylin levels in type 2 diabetes • cause or effect is unclear
Insulin and Glucagon Response to a Large Carbohydrate Meal in Type 2 Diabetes Depressed/delayed insulin response Nonsuppressed glucagon Type 2 diabetes mellitus (n=12)* Nondiabetic controls (n=11) 360 330 Meal 300 Glucose (mg/100 ml) 270 240 110 80 150 120 Insulin (µU/ml) 90 60 30 0 140 130 Glucagon (µµg/ml) 120 110 100 90 –60 0 60 120 180 240 Time (minutes) *Insulin measured in five patients Adapted from Müller WA et al N Engl J Med 1970;283:109–115.
Incretin Function in Type 2 Diabetes • Secretion of GLP-1 impaired • Beta-cell sensitivity to GLP-1 decreased • Secretion of GIP normal (or slightly impaired) • Effect of GIP abolished or grossly impaired Toft-Nielsen M-B et al. J Clin Endocrinol Metab. 2001;86:3717–3723; Kjems LL et al. Diabetes. 2003;52:380–386; Vilsbøll T et al. Diabetologia. 2002;45:1111–1119; Vilsbøll T et al. J Clin Endocrinol Metab. 2003;88:4897–4903.
The Pathophysiology of Type 2 Diabetes Includes Islet Cell Dysfunction and Insulin Resistance Liver Glucagon (Alpha cell) Pancreas Insulin (Beta cell) Glucose uptake Glucose output Hyperglycemia Muscle and adipose tissue Buse JB et al. In: Williams Textbook of Endocrinology. 10th ed. Saunders, 2003:1427–1483; Buchanan TA. Clin Ther. 2003;25(suppl B):B32–B46; Powers AC. In: Harrison’s Principles of Internal Medicine. 16th ed. McGraw-Hill, 2005:2152–2180; Rhodes CJ. Science. 2005;307:380–384. Adapted from Kahn CR, Saltiel AR. Joslin’s Diabetes Mellitus. 14th ed. Lippincott Williams & Wilkins; 2005:145–168.
Insulin Resistance • Genetics • Age • Weight • adipokines
Intra-abdominal adiposity is a major contributor to insulin resistance Associated with inflammatory markers (C-reactive protein) Free fatty acids Secretion of adipokines (↓ adiponectin) IAA = high risk fat Dyslipidaemia DM2 Increased cardiometabolic risk Insulin resistance Inflammation IAA: intra-abdominal adiposity Kershaw EE et al, 2004; Lee YH et al, 2005; Boden G et al, 2002
endocannabinoid system dysregulation Feeding ECS CB-1 blockade Weight Dyslipidaemia Type 2 diabetes Peripheral insulinresistance Hepatic insulinresistance Hepaticglucoseoutput Small,denseLDL-C LowHDL-C CETP,lipolysis Adiponectin Lipolysis FFA TG-richVLDL-C FFA Portal circulation ECS Liver Visceral fat ECS CB-1 blockade CB-1 blockade Weight-dependent Weight Independent Endocannabinoid system ECS Modified from: Lam TKT, 2003; Carr DB, 2004; Eckel R, 2005; Pagotto U, 2005; Di Marzo V et al, 2005 FFA=free fatty acids CETP=cholesterol ester transfer protein
Insulin Action • decrease in number of insulin receptors • any disruption in the transcription or transduction of insulin signaling pathway
Summary • Glucose metabolism is tightly regulated to maintain desirable glucose levels • Glucose dysregulation leads to progressive dysglycemia from prediabetes to frank diabetes • The pathophysiology of type 2 diabetes is complex. • Involves multiple physiologic and molecular disturbances influenced by multiple genes and environmental factors • This offers multiple target sites for therapy and explains the complexity of treatment of DM2