Download
1 / 43
450 likes | 840 Views
Interpretation of Periodontal Disease. Dr. Vandana Kumar BDS, MDS, MS. Periodontal disease. Gingival disease Periodontitis. Group of disease that affect surrounding and supporting tissues of teeth. Plaque induced. Non-plaque induced: Viral/fungal infections

E N D
Interpretation of Periodontal Disease Dr. Vandana Kumar BDS, MDS, MS
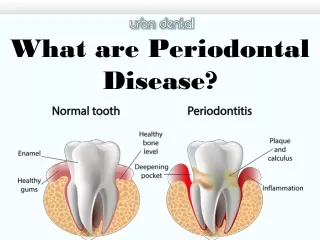
Periodontal disease • Gingival disease • Periodontitis Group of disease that affect surrounding and supporting tissues of teeth Plaque induced • Non-plaque induced: • Viral/fungal infections • Mucocutaneous/allergic reactions • Traumatic injuries Gingival inflammation Periodontal pocket formation Destruction of periodontal ligament Destruction of alveolar bone Gradual loosening of teeth
The causes of periodontal disease • Bacteria • Host related factors • Environmental factors
The result… • Chronic inflammation • Pocket formation • Apical migration of the epithelial attachment • Bone loss
The contribution of radiographs • Bone loss • Irritating factors • Crown/root ratio • Anatomic considerations • Pathologic considerations Condition of alv. crest Furcations PDL space Calculus Defective restorations Position of max. sinus Missing, supernumerary or impacted teeth Root morphology Crown/Root ratio Caries Periapical lesions
Limitations of radiographs… 1-Radiographs are 2D pictures of 3D structures 2-Radiographs show less severe bone destruction than is actually present 3-Do not show soft to hard tissue relationship, no information about depth of soft tissue pockets 4-Bone level measured from CEJ, Not valid in situations like severe attrition and passive eruption
Radiographs tend to show less severe destruction than is present
Alveolar ridge lies 1-1.5mm From CEJ of adjacent teeth
Alveolar crest pointed and well corticated
Classification • Early bone changes • Moderate bone changes • Advanced bone changes
Early bone changes • Loss of the crest’s cortication • Fuzzy appearance of the crest • Blunting of the crest in anterior teeth • 1-3 mm bone loss
Loss of the cortication of the alveolar ridge
Developing vertical defect Abnormal widening of PDL
Moderate bone changes • 3-5 mm bone loss • Horizontal bone loss • Vertical bone loss • Osseous defects
Developing vertical defect Abnormal widening of PDL
Evaluation of bone defects • Accurate radiograph shows bone defect in interseptal bone • Exact form and shape can be determined only by careful periodontal probing/ surgical exposure • Classification of infrabony pockets ( Goldman and Cohen in 1958) • One walled • Two walled • Three walled
Three walled defect Bony walls on three sides with tooth root forming fourth wall Not a circumferential defect Defect may extend around the root and stop on buccal/lingual aspect Two wall defect/ osseous craters Facial and lingual walls are intact But interdental alveolar crest is resorbed
Four wall bony defect Completely surrounds tooth One-wall bony defect One wall remains after the facial and lingual walls have been destroyed
One wall defect Facial & lingual walls destroyed One wall of interdental septum remains
Osseous crater/ Two wall bony defect Dry spiceman
Inconsistent bony margins
Advanced bone changes • Bone loss > 5 mm • Furcation involvement • Large bony defects • Periodontal abscess
One wall bony defect: Interdental bone slopes down From facial/lingual wall crest of bone toward crest of destroyed facial/lingual bone
Furcation involvement Furcation involvement
Recognition of Etiologic factors • Calculus deposits • Faulty restorations • Occlusal trauma • Tooth mobility • Aggressive periodontitis
Faulty restorations Open contacts Combined perio-endo pathosis #32