Download
1 / 41
540 likes | 4.99k Views
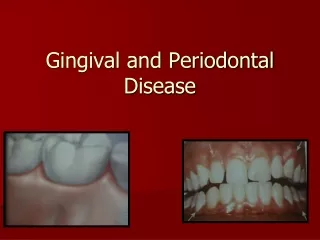
Gingival and Periodontal Disease. Introduction. Periodontium Gingiva Periodontal ligament: Cementum: Alveolar bone:. Classification. Plaque induced gingival diseases Gingivitis associated with dental plaque only Gingival disease modified by systemic factors

E N D
Introduction Periodontium • Gingiva • Periodontal ligament: • Cementum: • Alveolar bone:
Classification Plaque induced gingival diseases • Gingivitis associated with dental plaque only • Gingival disease modified by systemic factors 1) Associated with endocrine system a) Puberty associated gingivitis b) Pregnancy associated – Gingivitis , Pyogenic c) Diabetes mellitus associated gingivitis 2) Associated with blood dyscrasias a) leukemia associated gingivitis b) others American Academy of periodontology 1999
Gingival diseases modified by medications 1) Drugs influenced gingival diseases a) Drugs influenced gingival enlargement b) Drug influenced gingivitis- oral contraceptive associated gingivitis , others. • Gingival diseases modified by malnutrition 1) vitamin c deficiency gingivitis 2) others. American Academy of periodontology 1999
Gingival disease of specific bacterial origin. 1. Treponema pallidum 2. Streptococcal species Gingival disease of viral origin Herpes virus infections 1. Primary herpetic gingivostomatitis 2. Recurrent oral herpes 3. Varicella zoster Gingival disease of fungal origin Candida –species infection: Generalized gingival candidosis 2.Linear gingival erythema 3. Histoplasmosis. Gingival lesions of genetic origin. 1. Hereditary gingival fibromatosis. Gingival manifestations of systemic conditions. A. Mucocutaneous lesions. 1. Lichen planus. 2. Pemphigoid 3. Pemphigus vulgaris. 4. Erythema multiforme 5. Lupus erythematoses Non plaque induced gingival disease
B) Allergic reaction Dental restorative materials Mercury Nickel Acrylic Other 2) Reaction attributable to Tooth pastes or dentifrices Mouth rinses or washes Foods and additives Traumatic lesion Chemical injury Physical injury Thermal injury Foreign body reactions.
Gingivitis • Most common gingival disease - Gingivitis Gingivitis is the inflammation of the gingiva • Sequence of events in gingivitis – 4 stages Stage 1 gingivitis : The initial lesion Sub clinical gingivitis Initial manifestation - vascular changes – Dilation of capillaries and increased blood flow , infiltration of PMNs in junctional epithelium and gingival sulcus thus leading to an increase in the flow of gingival fluid into the sulcus.
Stage 2 gingivitis: Early lesion • Characterized by the presence of bleeding on probing. • Its due to proliferation of capillaries and increased formation of capillary loops between rete pegs. • Erythema is also seen. There is a increased in the amount of collagen destruction.
Stage 3 gingivitis the established lesion. • Chronic gingivitis where in the blood vessels become engorged and congested , venous return is impaired blood flow becomes sluggish. • Results in gingival anoxia bluish hue reddened gingiva
Stage 4 in gingivitis • Gingivitis is extended into the alveolar bone which leads to periodontal distruction.
Clinical features Based on course and duration • Acute gingivitis: Sudden onset, Short duration, Painful • Recurrent gingivitis : Reappears after treatment. • Chronic gingivitis : Slow onset, long duration, Painless Based on distribution • Localized gingivitis: Confined to single tooth or group of teeth • Generalized gingivitis: Gingivitis involves entire mouth.
Marginal gingivitis : Involve gingival margin • Papillary gingivitis: Involve Interdental papillae. • Diffuse gingivitis: Gingivitis affecting the gingival margin attached gingiva, and Interdental papillae.
Early symptoms of gingival inflammation Gingival crevicular fluid. Bleeding from gingival sulcus-probing Features: Gingival bleeding Color changes in gingiva Change in Consistency of gingiva Change in surface texture of gingiva Change in position of gingiva Change in gingival contor
Gingival recession • Apical migration of gingival margin- exposure of root surface • Presence of local factors • Improper brushing tech • Malposition • High frenal attachment • Soft tissue friction • Passing a probe over the exposed tooth surface might be highly sensitive to the patient
Acute gingival infections: • Necrotizing ulcerative gingivitis • Primary herpetic gingivostomatitis • Pericoronitis Necrotizing ulcerative gingivitis • Inflammatory destructive disease of the gingiva which presents characteristic signs and symptoms Predisposing factors • Change in living habit, work without rest, psychological stress, decreased immunity, poor oral hygiene , trauma
Oral signs: • Punched out crater like depressions at crest of Interdental papillae. • Extending into marginal gingiva rarely to attached gingiva & oral mucosa. • Craters are covered by grey pseudo membranous slough – linear erythema • Characteristic lesion destroy-Gingiva,Pdl • Spontaneous gingival hemorrhage, bleeding on slight stimulation. • Fetid odor, Increased salivation • Does not lead to Pdl pocket formation. • Rare in edentulous mouths. Oral Symptoms: • Sensitive to touch. c/o radiating pain. • Pain increase by hot and spicy. • Metallic foul taste
Extra oral systemic signs and symptoms : • Mild and moderate: Lymphadenopathy,slight elevation in temp. • Severe Systemic complication high fever, Pulse,leukocytosis Loss of appetite insomnia, GITdisturbances ,mental depression Prevalence : All age, 15- 30 yrs, socioeconomic group. D/D: Herpetic gingivostomatitis
Primary herpetic gingivostomatitis • HSV1 • Infants & children < 6 yrs age, m=f • Primary infection- asymptomatic. • Secondary manifestation – sunlight, trauma fever, stress • Herpes labials, Herpes genitalis, ocular Herpes and Herpetic encephalitis.
C/F: SIGNS • Diffuse erythematous shiny involvement of the gingiva & oral mucosa. • Gingival bleeding • Initial stage – Discrete spherical vesicles • After 24 hrs - vesicles rupture- painful ulcers red elevate halo like margin and depressed yellowish or grayish white portion • Occur in separate areas or in clusters, • Course of the disease- 7- 10 days ORAL symptoms • Generalized soreness- eating, drinking • Focal sites of pain, sensitive to touch, thermal changes
Extra oral and systemic signs & symptoms • Cervical lymphadenitis fever-101 f - 105 f, Malaise common. D/D : 1) Erythema multiforme 2) Stevens johnsons syndrome 3) Bullus lichen planus 4) recurrent aphthous stomatitis. It is a contagious Recurrence seen – Immunity destroyed
Pericoronitis • Inflammation of the gingiva in relation to the crown of the incompletely erupted teeth. • Commonly – Mand 3rd molar area • Acute , subacute , chronic C/F : • Markedly red swollen suppurating lesion – tender- radiating to ear, throat and floor of the mouth. • Foul taste experienced by patient. • Inability to open mouth with pain. • Swelling in cheek- In region of the angle of jaw, lymphadenitis are common Complication : Pericoronal abcess, Peritonsilar abscess ,Cellulitis, Ludwig's angina.
Systemic disease influencing gingival disease • Broadly its classified as • Nutritional deficiencies • Endocrine disorders • Hematological disorders • Immunodeficiency disorders • Cardiovascular disease Nutritional influence: • Vitamin deficiency: vita C – marginal gingiva is enlarged, bluish red, soft & friable & has smooth shiny appearance. surface necrosis with pseudo membrane formation
Endocrine disorders Diabetes mellitus • Influence of diabetes on Periodontium include a) Enlarged gingiva, sessile or Pedunculated gingival polyps, periodontitis. • Striking features in uncontrolled diabetes Reduction in defense mechanisms and the increased infection periodontal disease. • Periodontal disease in diabetics are: Severe gingival inflammation, deep periodontal pockets , rapid bone loss, frequent periodontal abscesses.
. Hematological disorders • Leukemia Leukemic infiltration , bleeding , oral ulceration and infection.
Anemia • Pernious anemia – tongue changes seen tongue appears red smooth shiny atrophy of the papillae. • Marked pallor of the gingiva • Iron deficiency anemia – tongue and gingival changes. • Sickle cell anemia – Generalized osteoporosis of jaw. • Aplastic anemia – pale discoloration of mucosa , infection • Thrombocytopenia – spontaneous bleeding into the skin or from mucous membranes, patechiae & hemorrhagic vesicles
AIDS • Characterized by destruction of lymphocytes thus rendering the person susceptible to opportunistic infection. • Destructive periodontal lesions NUP NUG and malignancies ( Kaposi's sarcoma) Cardiovascular disease Arteriosclerosis • Initmal thickening, narrowing of the lumen, thickening of the media ,hyalinization of the media • Vascular impairment Circulatory changes Patients susceptibility to Pdl disease.
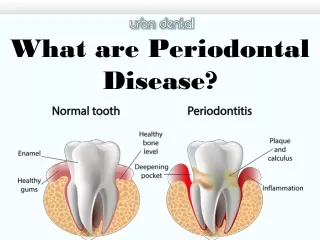
Periodontal pocket • Pathological deepening • True- as a result of destruction of adjacent periodontal tissue • False – gingival enlargement • PP can be assessed by gently walking a blunt probe within the gingival sulcus
PERIODONTITIS • DEFINITION:- An inflammatory disease of the supporting tissues of the teeth caused by specific microorganisms, resulting in progressive destruction of the periodontal ligament and alveolar bone with pocket formation , recession or both. • Attachment loss. • Classification :- 1) Chronic periodontitis 2) Aggressive periodontitis 3) Periodontitis as a manifestation of systemic diseases. Chronic periodontitis:- • Formerly Adult periodontitis. Can occur at any age. • Most prevalent form • Slow progressing • Clinical features :- Supra gingival and sub gingival plaque with calculus formation, gingival inflammation
Pocket formation, loss of periodontal attachment and loss of alveolar bone. • Gingiva is swollen and color ranging from pale red to magenta . Loss of stippling and blunted and rolled gingival margin. • Long standing cases , low grade inflammation , thickened , fibrotic marginal tissues . Pocket depth variable.Tooth mobility.Radiologically:-Horizontal or vertical bone loss can be seen.
Disease distribution: • Is a site specific disease • It can be described as Localized or Generalized. • Pattern of bone loss – vertical and horizontal • Disease severity :disease severity may be Slight (mild): 1-2 mm Moderate : 3-4 mm Severe : >5mm Symptoms • Usually painless ,Pain present in absence of caries,exposed roots sensitive to heat and cold, localized dull pain. Areas of food impaction – Discomfort to patient. • Gingival tenderness, itchiness may be present. Localized - < 30% Generalized-> 30%
Aggressive periodontitis • Describes 3 of the diseases formerly classified as early onset periodontitis 1) Localized aggressive periodontitis 2) Generalized aggressive periodontitis 3) Rapidly progressive periodontitis Localized aggressive periodontitis • C/F: Puberty, localized 1st molar/ incisors, - interproximal attachment loss 2 permanent teeth. • Striking feature – lack of clinical inflammation – Presence of deep pocket. • Plaque on affected teeth is minimal. • Age /sex: Male = female Puberty and 20 yrs
Disease progression : • Disease progress rapidly and the bone loss is 3-4 times faster than in CGP. • mobility. • sensitivity- Thermal and tactile stimuli. • Deep dull radiating pain – During mastication due to mobility • Pdl abcess – Regional lymph node enlargement may occur • Radiographic finding : Vertical loss of alveolar bone.
Generalized aggressive periodontitis : • Occurs < age 30 years. • Clinically it is characterized generalized interproximal attachment loss affecting at least 3 permanent teeth • Distruction appear to occur episodically – • Small amount of Bacterial plaque – Affected teeth. • Gingiva - Severe acutely inflamed tissue , Proliferating ulcerated and fiery red Bleeding may be spontaneous with slight provocation ,suppuration may be important feature, attachment and bone are actively lost.
Necrotizing ulcerative periodontitis • Extension of necrotizing ulcerative gingivitis into the periodontal structures, leading to attachment and bone loss. Signs and symptoms • Necrosis and ulceration of the coronal portion of Interdental papillae / gingival margin. • Painful ,bright red marginal gingiva that bleeds on even slight manipulation • Halitosis and systemic manifestations – fever malaise and lymphadenopathy
Periodontitis as a manifestation of systemic diseases Papillion lefevre syndrome • It is characterized by hyperkeratotic skin lesion. • Periodontal destruction. – bone loss , exfoliation of teeth • Calcification of the dura. • Primary teeth lost by 5-6 years. • Permanent teeth erupts , lost – 15 years. • Patients are edentulous except 3rd molars. • Inherited as autosomal recessive
Down syndrome • It is a chromosomal abnormality, congenital disease. characterized by mental deficiency and growth retardation. • Prevalence of pdl disease in down syndrome is high (100%). • Deep PDL pockets with substantial plaque, moderate gingivitis. • Features are generalized but > in lower anterior. • ANUG are frequent findings. • Progression is Rapid.
Periodontal abcess (Lateral or parietal abcess) • It is a localized purulent inflammation in the periodontal tissues. • Infection from Pdl pockets. • In absence of Pdl disease after trauma to the teeth Organisms- gram – ve anaerobic rods. Periodontal abcess are classified according to location • Abscess in the supporting periodontal tissue. • Abscess in the soft tissue wall – Deep pocket.
Gingival abscess • Embedding of foreign objects into the gingiva • Marginal or inter dental • Can occur in the absence of pocket, and mobility • Pus discharge absent • No radiographic findings
Conclusion • Gingival diseases and periodontal diseases are commonly seen in daily practice • For proper diagnosing and treating the gingival and Periodontal diseases a sound knowledge of disease , their C/F , and radiological features are necessary.
Questions • Difference between gingival and periodontal abscess • Periodontal Pockets • Clinical Signs of Gingival and Periodontal diseases • Clinical examination of Patients with Gingival and periodontal diseases • Classify Gingival and periodontal diseases