Download

1 / 35
350 likes | 479 Views
GRAFT Thrombosis: Recent trends in Management. Introduction. Most patients with end-stage renal disease undergo hemodialysis thrice weekly to Optimize their survival Minimize medical complications and Enhance their quality of life A reliable vascular access is a

E N D
Introduction • Most patients with end-stage renal disease undergo hemodialysis thrice weekly to • Optimize their survival • Minimize medical complications and • Enhance their quality of life • A reliable vascular access is a • Critical requirement for providing adequate hemodialysis
Introduction • The ideal vascular access would be • Easy to place • Ready to use as soon as it is placed, • Deliver high blood flows indefinitely, and • Free of complications • None of the existing types of vascular access achieves this ideal • Among the three types of vascular access currently available, • Native arteriovenous (AV) fistulas are superior to AV grafts, which, in turn, are superior to dialysis catheters
Introduction • Recognizing the relative merits of the vascular access types, the Kidney Disease Outcomes Quality Initiative (K/DOQI) guidelines recommend placement of • AV fistulas in at least 50% of hemodialysis patients, • AV grafts in 40%, and • Dialysis catheters in no more than 10%
SPECIFIC CRITERIA PTFE A-V Graft Autologous options have been considered / excluded / exhausted (Exception : graft first may preserve future options) Absence of Collagen Vascular Disease (Lupus Nephritis) Generally, forearm before upper arm (Exception : secondary upper arm graft on non-dominant side) Superficial vein target preferable to deep vein Min diam of venous target >4.5 mm, min length > 16 mm Success upper arm graft limited if diam < 5 mm Arterial target diam > 3.5 mm (4.0 mm upper arm) Consider 5 mm graft Consider crossing joint
Introduction • Vascular access procedures and their subsequent complications represent a major cause of • Morbidity, • Hospitalization, and • Cost for chronic hemodialysis patients
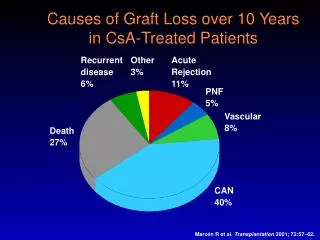
AV grafts • AV grafts are prone to • Recurrent stenosis and thrombosis and • Require multiple radiologic or surgical interventions to ensure their long-term patency for dialysis
AV graft thrombosis • About 80% of graft failures are due to thrombosis • Thus, improving graft longevity requires implementing measures to reduce the frequency of graft thrombosis • When grafts are referred for thrombectomy, a significant underlying stenosis is observed, most commonly at the venous anastomosis, the draining vein, or the central veins • This observation suggests that • Prophylactic angioplasty of hemodynamically significant graft stenosis may reduce the frequency of graft thrombosis, and thereby increase cumulative graft survival
AV graft thrombosis • Thrombosed grafts usually have an underlying stenosis, • most commonly at the venous anastomosis or in the draining vein • Salvage of clotted grafts requires • Thrombectomy as well as • Angioplasty or surgical revision of the underlying stenosis
AV graft thrombosis • However, the primary patency (intervention free survival) is considerably worse after treatment of clotted grafts, as compared with • Elective angioplasty of patent grafts with stenosis • After elective angioplasty, the primary graft patency is • 70 to 85% at 3 mo and 47 to 63% at 6 mo • In contrast, after thrombectomy and angioplasty of clotted grafts, the primary patency is only • 33 to 63% at 3mo and 11 to 39% at 6 mo
AV graft thrombosis • Comparison of outcomes of 656 radiologic graft interventions performed at a single dialysis center found a 3-mo primary patency of • 71% after elective angioplasty, as compared with • 30% after treatment of clotted grafts Am J Kidney Dis 2001;37: 945–953
AV graft thrombosis • Given the dismal outcomes of clotted grafts, it would be desirable to • Identify prospectively grafts that are at risk for thrombosis and intervene prophylactically to prevent the graft from clotting • Because graft thrombosis is usually superimposed on hemodynamically significant stenosis, it is a plausible hypothesis that timely detection and correction of the stenosis will prevent graft thrombosis Clin J Am Soc Nephrol 2007;2: 786–800
AV graft thrombosis • Achieving this goal requires having a • Simple • Cheap • Reproducible, and • Sensitive method to • Monitor for graft stenosis Clin J Am Soc Nephrol 2007;2: 786–800
Mechanical Interventions to Reduce Graft Thrombosis • Approaches for detection of graft stenosis • Clinical monitoring consists of physical examination (absent thrill, abnormal bruit, or distal edema), • Abnormalities identified during dialysis sessions • Prolonged bleeding from needle sites or • Difficulty in cannulation), or • An unexplained decrease in Kt/V on a constant dialysis prescription Clin J Am Soc Nephrol 2007;2: 786–800
NKF KDOQI GUIDELINES 2006 Updates Vascular Access • AVGs have the following advantages: • A large surface area and vessel available for cannulation initially • They are technically easy to cannulate • The lag-time from insertion to maturation is short • For PTFE-derived grafts, it is recommended that not less than 14 days should elapse before cannulation to allow healing and incorporation of the graft into local tissues, although ideally, 3 to 6 weeks are recommended • Multiple insertion sites are available
NKF KDOQI GUIDELINES 2006 Updates Vascular Access • AVGs have the following advantages: • A variety of shapes and configurations is available to facilitate placement • It is easy for the surgeon to handle, implant, and construct the vascular anastomosis • The graft is comparatively easy to repair either surgicallyor endovascularly
NKF KDOQI GUIDELINES 2006 Updates Vascular Access • The sum of the available data, until recently, supported PTFE grafts over other biological and other synthetic materials, based on • lower risk for disintegration with infection, longer patency, better availability, and improved surgical handling • Biological grafts (bovine heterografts) have greater reported rates of complications compared with synthetic grafts
NKF KDOQI GUIDELINES 2006 Updates Vascular Access • For nearly 2 decades, • PTFE has been the material of choice for bridge grafts. • However, during the past decade, modificationsand the use of other materials, such as PU,cryopreserved femoral vein,bovine mesenteric vein, and hybrids with self-sealing composite material, have been developed and used • None of these has shown any “survival” patency over plain PTFE, except for the composite/PU graft
NKF KDOQI GUIDELINES 2006 Updates Vascular Access • Composite/PU graft • Has an advantage because of its self-sealing property to be cannulated within hours, if needed, for dialysis • As a result, it can be placed without having to use a catheter for initiation of dialysis therapy, in some cases • Direct comparisons between PTFE and human umbilical cord vein grafts and other synthetic polymers have not been made
NKF KDOQI GUIDELINES 2006 Updates Vascular Access • Treatment of thrombosis and associated stenosis:Each institution should determine which procedure, percutaneousthrombectomy with angioplasty or surgical thrombectomy with AVG revision, is preferable based upon expediency and physician expertise at that center. • 6.7.1 Treatment of AVG thrombosis should be performed urgently to minimize the need for a temporary HD catheter. (B) • 6.7.2 Treatment of AVG thrombosis can be performed by using either percutaneous or surgical techniques. Local or regional anesthesia should be used for the majority of patients. (B) • 6.7.3 The thrombectomy procedure can be performed in either an outpatient or inpatient environment. (B)
NKF KDOQI GUIDELINES 2006 Updates Vascular Access • 6.7.4 Ideally, the AVG and native veins should be evaluated by using intraprocedural imaging. (B) • 6.7.5 Stenoses should be corrected by using angioplasty or surgical revision. (B) • 6.7.6 Methods for monitoring or surveillance of AVG abnormalities that are used to screen for venous stenosis should return to normal after intervention. (B)
NKF KDOQI GUIDELINES 2006 Updates Vascular Access • Outcomes after treatment of AVG thrombosis:After percutaneous or surgical thrombectomy, each institution should monitor the outcome of treatment on the basis of AVG patency. Reasonable goals are as follows: • 6.8.1 A clinical success rate of 85%; clinical success is defined as the ability to use the AVG for at least 1 HD treatment. (B) • 6.8.2 After percutaneousthrombectomy, primary patency should be 40% at 3 months. (B) • 6.8.3 After surgical thrombectomy, primary patency should be 50% at 6 months and 40% at 1 year. (B)
Options for treating steal DRIL procedure distal revascularization-interval ligation excision of a portion of the vein plication w/ mattress or continuous sutures crossed PTFE band interposition of a 4 mm PTFE
Venous angioplasty Graft thrombolysis Treatment of venous access complications.
Contraindications to Thrombolytic Therapy • Absolute Recent major bleeding Recent stroke Recent major surgery or trauma Irreversible ischemia of end organ Intracranial pathology Recent ophthalmologic procedure • Relative History of gastrointestinal bleeding or active peptic ulcer disease Underlying coagulation abnormalities Uncontrolled hypertension Pregnancy Hemorrhagic retinopathy
Recent articles • Patency rate and complications of polytetrafluoroethylene grafts compared with polyurethane grafts for hemodialysis access. • RESULTS: • One-year patency rate was reported to be 64% and 52% in the PTFE and PVAG groups, respectively. There was no significant difference in 1-year (64% versus 52%) and 2-year (49% versus 41%) patency rate of the PTFE and PVAG grafts used as vascular access. There was also no difference between the numbers of complications reported in the two groups. • CONCLUSION: • It could be concluded that either PTFE or PVAG grafts can be used with the same expected outcomes • Ups J Med Sci. 2010 Nov;115(4):245-8
Long-term Outcome of a Cuffed Expanded PTFE Graft for Hemodialysis Vascular Access • Compared to the standard ePTFE, the cuffed ePTFE graft provided better long-term outcome, especially in terms of secondary patency rates after radiological intervention World Journal of SurgeryVolume 32, Number 8, 1827-1831
Balloon Angioplasty Versus Surgical Revision for Thrombosed Dialysis Graft Outlet Stenosis After Graft Thrombectomy • The result of dialysis graft outlet balloon angioplasty was comparable to that of surgical revision. Considering the invasiveness, balloon angioplasty should be considered when treating thrombosed dialysis grafts. ANGIOLOGY August 2010; 61 (6):580-583
LifeSite ® 12 F. Catheter Multi-side-hole tip