Download

1 / 1
10 likes | 94 Views
Explore the case study of a patient with moderate haemophilia B, detailing genetic studies, inhibitor formation, treatment with FIX concentrates, and proposed assay modifications for accurate FIX activity testing. Discover the challenges faced in measurement and inhibitor testing.

E N D
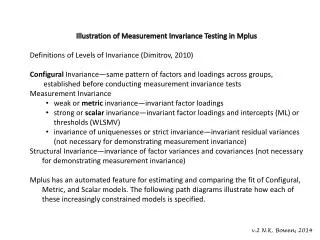
Silvana Spiteri, Kevin Vella, Alex Gatt Haematology and Coagulation, Department of Pathology 1st Applied Biomedical Science Meeting 20th Anniversary Introduction Haemophilia B (Christmas disease) is characterised by low levels of coagulation factor IX (FIX). It is the second most common bleeding disorder that is inherited as an X-linked recessive trait. The incidence is 1:30,000 males and whilst female carriers are usually unaffected, they can be carriers. Over 300 gene mutations have been identified; most commonly being single point mutations. The classification of the disease depends entirely on the FIX activity; mild (>5%), moderate (1-5%), and severe (<1% activity). The clinical features are bleeding into soft tissue, joints or muscle, easy bruising and excessive bleeding after trauma. Chronic complications of haemophilia B include transfusion-related infections, musculoskeletal problems and FIX inhibitor formation. The formation of inhibitors leads to ineffective therapy, thus increasing the incidence of bleeding episodes. Case Summary Our patient presented with multiple large subcutaneous haematomas. Laboratory findings at time of presentation were as follows: • FIX result also confirmed with a reference laboratory (3% FIX activity) • Indicating a case of moderate haemophilia B • Genetic studies revealing a complete FIX gene deletion • Patient treated with plasma derived FIX concentrates as prophylaxis • After around 20 exposure days he developed a low level inhibitor of 0.95 Bethesda units/ml. He was treated with a bypassing agent (Novoseven) until the inhibitor disappeared and then changed back to pdFIX (plasma derived FIX) concentrates and has had more than 50 exposure days to date without any problems Limitations in FIX Measurement and Inhibitor Testing Table 1: Coagulation tests revealing a prolonged APTT corrected with mixing studies and low levels of FIX activity Measurement of FIX Measurement of FIX Inhibitors Limitations • FIX deficient plasma has 1% FIX activity (unsuitable for our case scenario) • Current Bethesda assay has a detection threshold of 0.6% (not suitable for early detection of inhibitor) • Deficiency of FIX results in a prolonged APTT • FIX levels determined by performing an APTT as shown in figure 1 • Calibration curve using serial dilutions of standard human plasma (SHP) (table 2) • Figure 2 shows the test procedure of FIX inhibitor • Corrected percent residual activity FIX activity (B)/FIX activity (A) X 100% • 1 Bethesda unit (BU) is the amount that neutralises 50% of 1 unit of FIX Proposed assay modification • Increasing the serial dilutions of the calibration curve up to 1:256 will increase the accuracy of FIX activity up to 0.387%. This has already been done and FIX activity levels of 0.3% were determined. • FIX activity in the deficient plasma has been measured and subtracted from patients results (blank) • The Nijmegen modification of the Bethesda assay involves the serial dilution of patient’s plasma thus giving the possibility to detect the early formation of inhibitors. Table 2: SHP serial dilutions utilised for FIX calibration Fig. 2: Schematic representation for Bethesda assay for FIX inhibitor Conclusion • The current test for FIX activity permits the screening for possible haemophilia B patients • It is not suited for severe haemophilia patients due to the undetectable FIX activity levels in such cases • ELISA and Western Blots have been used in such cases but probably not feasible or cost effective situation locally • Further validation of proposed assay modifications are warranted to assess suitability Fig. 1: Schematic representation for determination of FIX activity Fig. 3: Graph showing the corrected residual FIX vs the Bethesda units