Download
1 / 23

E N D
ABG IN THE EYE OF ELETROLYTES….!!! Dr Vishram Buche Dept of pediatric Intensive Care Central India”s Child Hospital and Research Institute Nagpur Ex-National Chairman Pediatric Intensive Care Chapter
Approach to ABG Interpretation………………….. AND ELECTROLYTES Assessment of Oxygenation ventilatory Status Assessment of Acid-Base Status Volume Osmolality Electrolytes There is an interrelationship, but less confusing if considered separately…..
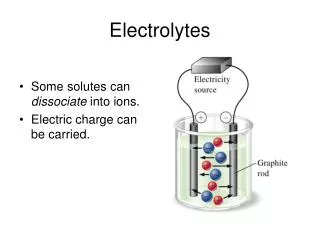
An asymptomatic patient is found to have the following laboratory values: • Na+ ……142 mEq/L • K+ ……3.0 mEq/L • Cl- ……112 mEq/L • HCO3 ……14 mEq/L • MOST LIKELY CULPRIT?
K Cl Na Poor man’s pH meter ANION Gap HCO3 Delta Gap Urinary Gap U-Na U-Cl
K • ELECTROLYTES ……………. • 1 Diagnosing acid base disorder/ acidosis, alkalosis • 2 Differential diagnosis • 3 Diagnosing specific cause disease • 4 Monitoring disease progress/ resolution of a disease • 5 Crucial management of a disease • 6 Oxygen delivery..? Poor man’s pH meter Cl Na ANION Gap HCO3 Delta Gap U Gap U-Na U-Cl
DIAGNOSTIC UTILITIES OF ELECTROLYTES ………………………. K+ HCO3- Chlorides ANION GAP
K+ Typical K changes in acid –base disorders……… N N CHRONIC A C U T E N • Metabolic … Acidosis…. cause specific ………. ↑ or N In DKA n Lactic acidosis….. • ↓… Diarrhoea, RTA1 n 2 • ↑… in RTA 4 Acidosis Alkalosis Acidosis Alkalosis Metabolic Respiratory
DIAGNOSTIC UTILITIES OF ELECTROLYTES ………………………. Sometimes it is aptly said that……… is Poor man’spH meter…….!!!!! K+ HCO3- K Chlorides ANION GAP
DIAGNOSTIC UTILITIES OF ELECTROLYTES ………………………. HCO3- HCO3………………..22-26 Abnormal HCO3 ……..Acid base disorder Metabolic …………….Direct effect Respiratory ………….Indirect effect History………HCO3…… 36…………Meta alkalosis 36 ……….. Resp acidosis 17 ……….. Hepatic failure 24 ………... Abnormal ??
DIAGNOSTIC UTILITIES OF ELECTROLYTES ………………………. K+ HCO3- Which HCO3………?? Calculated? Measured? Actual? Standard …….?? Chlorides ANION GAP
DIAGNOSTIC UTILITIES OF ELECTROLYTES ………………………. ANION GAP AG = Na – (HCO3 +Cl) Anion Gap / Delta Gap…………….tools to…….. • Diagnose ……………………. ABG report normal • Differential Diagnosis.. • Cause of acidosis………….. .N--AG / ↑AG • Monitor disease Process …..AG…….DKA • Delta Gap …….(only in ↑ AG acidosis)…. …………..additional metabolic disorder Its good idea to measure ELECTROLYTES with every ABG
DIAGNOSTIC UTILITIES OF ELECTROLYTES ………………………. K+ HCO3- Urinary GAP Chlorides ANION GAP Urine Na/Cl
Cause specific Diagnosis of N-AG Met Acidosis Urine Na/Cl Urinary GAP Urine Na Cl Supporting Meta Alkalosis Is there any way to differentiate………?? Combined case of RTA and Diarrhoea…….??
Use of the Urine Anion Gap (UAG) in Normal AG AcidosisBatlle et al. NEJM 318:594, 1988 Urine AG = (Na + K) - Cl • -ve UAG = Normal, or GI loss of HCO3 • +ve UAG = altered distal renal acidification • Caveats: Less accurate in patients with volume depletion (↓ U Na); and in patients with increased excretion of unmeasured anions (e.g. ketoacidosis), where there is increased excretion of Na and K to maintain electroneutrality)
Use of the Urinary AG in Normal Gap AcidosisBatlle et al. NEJM 318:594, 1988 Plasma KUAG U pHDiagnosis Normal - < 5.5 Normal Normal-low - < 5.5 GI HCO3 loss High + < 5.5 Aldo deficiency High + > 5.5 Distal RTA Normal-low + > 5.5 Proximal RTA
Lab Report 1…………………… Na …….. 143 K ………..3.2 Cl ……….91 HCO3 …. 40 Low K High HCO3 1.Metabolic Alkalosis OR 2. Compensated Resp Acidosis N…Anion Gap = 143 – (94+40) = 9 And HypoChloremia……!!! Metabolic Alkalosis…………!!!
Lab Report 2…………………… Na …….. 140 K ………..3.0 Cl ……….115 HCO3 …. 15 Low K LOW HCO3 1.Metabolic Acidosis OR 2.Compensated Resp alkalosis N..Anion Gap = 140 – (115+15) = 4 And hyperChloremica…….!!! Metabolic Acidosis……………..!!!!
Lab Report 3…………………… Na …….. 145 K ………..3.2 Cl ……….81 HCO3 …. 34 Low K HIGH HCO3 1.Metabolic Alkalosis OR 2.Compensated Resp acidosis ↑ Anion Gap = 145 – (81+34) = 30 And HypoChloremia Mixed Metabolic Acidosis + Alkalosis
An asymptomatic patient is found to have the following laboratory values: • Na+ ……142 mEq/L • K+ ……3.0 mEq/L • Cl- ……114 mEq/L • HCO3 ……14 mEq/L • MOST LIKELY CULPRIT? ↓ HOC3 ↓ K Anion Gap ….normal 142-(114+14) = 14 ↑ Chlorides RTA
TAKE HOME MESSAGE……………………… Its good idea to measure ELECTROLYTES with every ABG Always correlate ABG and electrolytes report clinically.
There is no copyright on this material….please copy for educational purposes…. Visit me on…………… www.slideshare.net www.authorstream.com THANKS For any queries : vbuche@gmail.com Cell : 9823017254