Download
1 / 39
390 likes | 414 Views
Explore advances in risk assessment through collaboration, transparency, and harmonization via the Alliance for Risk Assessment Beyond Science and Decisions workshops. Learn about the case study process, dose-response framework, and the Alliance's qualitative and quantitative assessment methods.

E N D
Problem Formulation to Dose-Response: Advances via the Alliance for Risk AssessmentBeyond Science and Decisions Workshops Michael DoursonToxicology Excellence for Risk Assessment
Alliance for Risk Assessmentwww.allianceforrisk.org • A collaboration of organizations dedicated working together to solve public health issues • Improve communication among groups • Provide transparency in development of products • Foster harmonization and consistency in risk assessments • Share costs and human resources
ARA Science Panel • Michael Bolger, U.S. Food and Drug Administration • James S. Bus, The Dow Chemical Company • John Christopher, CH2M/Hill • Rory Conolly, U.S. Environmental Protection Agency • Michael Dourson, Toxicology Excellence for Risk Assessment • *Adam M. Finkel, UMDNJ School of Public Health • William Hayes, Indiana DEM • R. Jeffrey Lewis, ExxonMobil Biomedical Sciences, Inc. • Randy Manning, Georgia Department of Natural Resources • Bette Meek, University of Ottawa (Chairperson) • Paul Moyer, Minnesota Department of Health (MDH) • *Greg Paoli, Risk Sciences International • Rita Schoeny, U.S. Environmental Protection Agency • *On NAS Science and Decisions panel
Case Study Process • Engagement from wide variety of stakeholders • Proposed in brainstorming prior to first workshop • Initial vetting in breakout groups at 1st workshop • Presentations at 2nd workshop • Additional case studies identified at 2nd workshop • 30+ case studies proposed • 24 case studies presented and reviewed by panel
Case Study Process & Dose-Response Framework • Organization of methods and ability to identify gaps into an interactive framework based on NAS (2009): Problem formulation DR method Management decision • The framework was developed by the panel after review of all case studies in the 2nd workshop, and was used to prioritize new case studies for 3rd workshop, focusing on 3 topic areas: • Problem formulation • Mode of action • Endogenous & background exposures
Science and Decisions, NAS (2009) Framework for Risk Assessment Formulate Problem Plan & Conduct Manage Risk • Determine problems with conditions • Determine options for change • What assessments are necessary for risk options? • Plan assessment • Conduct: • Hazard ID • DR assessment • Exposure assessment • Risk characterization • Confirm Utility • Determine: • Option benefits • How options affect other decision factors • Justify decision re benefit, cost & uncertainty • Communicate decision
Alliance for Risk Assessment (ARA): Beyond Science and Decisions Workshop Series PHASE 1: Problem Formulation & Scoping [Adapted from NAS (2009) Figure S-1] What problems are associated with existing environmental conditions? If existing exposure conditions appear to pose a threat to human or environmental health, what options exist for altering those conditions? Under the given decision context, what risk and other technical assessments are needed to evaluate possible risk management options? Qualitative Decision Quantitative Screening In-Depth Assessment
ARA: Beyond Science & Decisions Qualitative Decision • Exposure and Endpoint Assessment • Identify potential health effects • Consider strengths and uncertainties in data • Identify potential exposure scenarios Health Assessment Use available data to assist management decision Vulnerable Populations Assessment Use available data to assist management decision Exposure Assessment Use available data to assist management decision Integration Results Reporting
ARA: Beyond Science & Decisions Quantitative Screening Decision • Exposure and Endpoint Assessment • Identify adverse effects and chemical mode of action • Determine strengths and uncertainties in data • Define exposure scenarios; get data on exposed populations Health Assessment Use available data to determine critical effect & action mode Vulnerable Populations Assessment Use available data to determine potential groups at risk Exposure Assessment Use available data to determine upper bound exposures Exposure & Dose-Response Evaluation Based on the available information, estimate a health-protective exposure limit Results Reporting
Quantitative Screening Decision • Tiered approach case study • Low-dose Extrapolation from BMD(L) • Threshold of toxicological concern/ of regulation • Screening-level safe dose (e.g., RfD) • Structure-activity relationships and read-across Quantitative SAR
ARA: Beyond Science & Decisions In-Depth Assessment • Exposure and Endpoint Assessment • Identify adverse effects and their precursors and MOA • Identify exposures, endpoints or lifestages under-assessed • Identify probabilistic exposure scenarios focusing on vulnerable populations Health Assessment Chose appropriate extrapolation based on MOAs and background disease Vulnerable Populations Assessment Identify vulnerable groups, considering exposures, endpoints and MOA Exposure Assessment Identify endogenous exposures & conduct probabilistic exposure scenarios Risk Characterization Integrated extrapolation with probabilistic exposure based on vulnerable populations Communicate characterization with uncertainties
Dose Response Framework The risk assessor is guided to methods that address key issues, such as: • Mode of action assessment • Vulnerable population assessment • Endogenous/background exposure • Dose-response methods reflecting different • Conceptual models • Data availability • Risk management needs
Methods Linked to Real-World Application • Summaries that • briefly describe dose response method, • provide references, • outline data requirements, • describe strengths and weaknesses • In depth full case study • Workshop presentation slides
The Expert Panel Determined… • A wide range of problem formulations exist for which different dose-response analysis techniques are needed. • Risk assessors must explain criteria applied in the choice of a particular dose-response method, and how results will be used in a risk management decision. • Additional case studies would be useful on topics such as: • Combined exposures • Value of information • Illustrating an entire risk assessment, from problem formulation to conclusion • In vitro to in vivo extrapolation
Next Steps • Framework will be “evergreen” • Updated with additional methods illustrated by case studies, and • Papers developed addressing & resolving cross-cutting issues. • The National Library of Medicine is hosting the Framework. • A standing panel will be created to meet twice a year to review additional case studies and issue/resolution papers. • Additional sponsors/participants will be invited to join in the overall effort.
Framework • ARA Dose Response Framework – (working beta) http://www.allianceforrisk.org/workshop/framework/ problemformulation.html • Part 2 of the symposium presents several sample methods and case studies for risk around the RfD
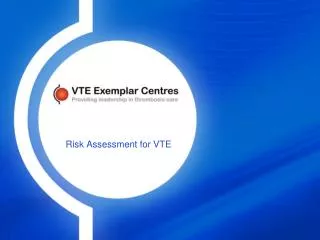
ARA Cases on Risk Around the RfD Areas of Uncertainty to Consider in Noncancer Dose Response Assessment Sub-chronic Animal 1 Chronic Human Chronic Animal Response Reproductive LOAELs UFL UFS UFD PBPK NOAELs or BMDs 0.1 UFH UFA Dose
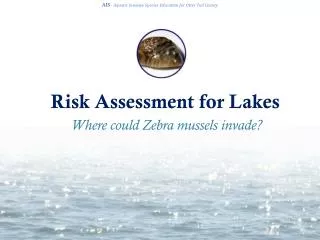
Case Study 17: Oliver Kroner & Lynne Haber, TERA *This case study is a characterization of the method, and is not intended as endorsement or opposition of linear extrapolation. Methods 1 to 4: extend a straight line from the chosen BMD or BMDL adjusted to the human equivalent dose or concentration (HED or HEC) by default or modified uncertaintyfactors. Method 5: linearize HED(C) dose-response data using probit transformation in logarithmic space. Fit regression line to the data and extend to the low-dose
Method 1: Linear extrapolation from BMD Response Animal BMD Human Equivalent Dose UFS UFD UFA 0.1 Dose
Factor of 10 Enough? Dourson, M.L., G. Charnley and R. Scheuplein, 2002
Strengths and Limitations • Strengths • Simple to use and provides risk at any dose • Limitations • No consideration of underlying Mode of Action • Depending on UF, risk could be highly conservative • ARA Science Panel Comments • Possibly useful for screening, but should not be construed as accurate estimate of risk • Requested exploration of non-cancer linear extrapolation in log-dose, probit space
Probit Transformation • Linearizes biological data • Requires population data • To allow graphing in log space, response rates were converted to Excess Risk [added risk(d) = P(d) - P(0)] for each dose group • a dataset of at least three test doses above the control From Casarett & Doull 2009
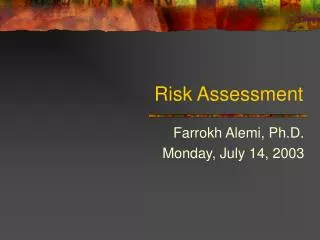
Method 5: Linear Extrapolation in Log-Dose, Probit Space Probit Response Animal Data Human Equivalent Dose 5 UFS UFD UFA Log Dose
Probit Response Log(10) Dose
Strengths and Limitations • Strengths • Simple, and provides risk at any dose • Consistent with toxicological theory of probit/logarithmic dose response • Limitations • Restrictive data requirements permitted the use of only 4 of 25 chemicals; such restriction could be relaxed • Differing results may be due to expected differences among chemicals in adverse responses, or different amounts of dose response data.
Case Study 11:Elizabeth Spalt, IDEM & Oliver Kroner, TERA • Straightforward application of Swartout et al. (1998). • A single distribution is assumed for all factors, specifically, lognormal with a median of 100.5and a 95th% value of 10. • Various probabilities of Swartout et al. (1998) are combined by multiplication. Other combinations may be possible. • Method indirectly addresses recommendation of NAS (2009) to develop probabilities for RfDs, but probabilities state whether RfD is correctly identified as a sensitive human NOAEL or BMDL.
Comparison of RfD Values for Three Compounds with an IRIS RfD of 0.03
Strengths and Limitations • Strengths • Method shows how different factors result in RfDs with different probabilities of being correctly identified as a sensitive human NOAEL. • Method is straightforward and simple and can be used to judge among given RfDs or used to standardize all RfDs. • Limitations • Method assumes a similar distribution for all factors; although conservative, it may not represent all chemicals. • The probability is the likelihood that the stated RfD is a sensitive human NOAEL, rather than describing the probability of a response in a population.
Case Study #21Robinan Gentry & Cynthia Van Landingham, Environ;Lesa Aylward & Sean Hays, Summit • Extension of the Benchmark Dose (BMD) method • Development of risk values at doses above the Reference Dose (RfD) • Methylmercury – Dose-response information in humans – BMDs estimated using biomarkers (i.e., levels in hair and cord blood) – Multiple BMDs available – Sensitive human subpopulation (children exposed in utero)
4 Approaches • Approach 1 - A straight line is drawn from both the BMDL and BMD to the RfD, where the RfD is considered to be zero risk; • Approach 2 - The appropriate BMD model is extrapolated to the RfD and then the risk at the RfD is truncated to zero; • Approach 3 - The appropriate BMD model is extrapolated to the RfD and this risk is allowed to stand as an upper bound; • Approach 4 - The appropriate BMD model is extrapolated using a threshold term, where the threshold value is judged to be the RfD, or some higher value.
2 BMDL 1 BMDL 1 BMD 3 BMDL 3 BMD 2 BMD
Strengths and Limitations • Strengths: • Use of a biomarkers, typically closer to the “target tissue” • Ability to evaluate the potential fraction of people exposed above and below the RfD to assess the likelihood of adverse effects • internal concentration may be extended to an exposure level • Limitations: • Uncertainties for other compounds as to the relationship between biomarker and effects of concern • Information characterizing the potential shape of the dose-response curve below the BMD/BMDL
Summary • A wide range of problems exist for which different dose-response methods and case studies are needed: • Combined exposures • Value of information • Illustrating an entire risk assessment • In vitro to in vivo extrapolation • Assessors must explain choice of a particular method and its usefulness in a management decision. • A standing panel is being formed to review additional methods, case studies and issue/resolution papers. • Additional folks are invited to join the effort.