Download

1 / 51
520 likes | 692 Views
Drugs for leukemia and lymphoma. Pharmacology tanghuifang@zju.edu.cn 2012-3-5. overview. 造血器官和组织可以发生恶性肿瘤,发生的原因与各种理化因素对机体的刺激、病毒的感染及个体的遗传因素有关。 常见的恶性肿瘤有 白血病和淋巴瘤 。出血、感染、贫血和肝脾淋巴结肿大是这类疾病常见的症状。. Definition of Leukemia.

E N D
Drugs for leukemia and lymphoma Pharmacology tanghuifang@zju.edu.cn 2012-3-5
overview • 造血器官和组织可以发生恶性肿瘤,发生的原因与各种理化因素对机体的刺激、病毒的感染及个体的遗传因素有关。 • 常见的恶性肿瘤有白血病和淋巴瘤。出血、感染、贫血和肝脾淋巴结肿大是这类疾病常见的症状。
Definition of Leukemia • 白血病:这是一类造血干细胞的克隆性恶性疾病,白血病细胞失去进一步分化和成熟的能力而停滞在细胞发育的不同阶段。骨髓和其他造血组织中白血病细胞大量增生积聚,浸润其他器官和组织,使正常造血受到抑制。
Classification of Leukemia • 根据起病缓急和白血病细胞发育停滞的阶段,可以将白血病分为急性与慢性。 • 急性类型的白血病细胞类似原始或早幼细胞, • 慢性白血病细胞接近成熟白细胞。 • 根据主要受累的细胞系列,可以将白血病分为 • 淋巴细胞白血病( lymphocytic leukemia ) • 髓系细胞白血病( myelocytic leukemia) • 根据增生细胞的类型可分为淋巴细胞性和粒细胞性白血病两类。
Type of Leukemia • Acute: • 急性淋巴细胞性白血病(acute lymphocytic leukemia,ALL) • 急性粒细胞性白血病(acute myelocytic leukemia,AML)或急性非淋巴细胞性白血病(acute non-lymphocytic leukemia,ANLL), • Chronic: • 慢性粒细胞性白血病(chronic myelocytic leukemia,CML)。 • 慢性淋巴细胞性白血病(chronic lymphocytic leukemia,CLL),
Type of Acute Leukemia FAB分类 • 急性淋巴细胞性白血病(ALL)可分为:3个亚型; • L1(小细胞为主), • L2(混合细胞、大细胞为主), • L3(大细胞为主,Burkitt型) • 急非淋巴细胞(ANLL)可分为: 7种亚型。 • M1(原始粒细胞白血病未分化型)、 • M2(原始粒细胞白血病部分分化型)、 • M3(早幼粒细胞白血病)、 • M4(粒一单核细胞白血病)、 • M5(单核细胞白血病)、 • M6(红白血病)、 • M7(巨核细胞白血病)
急性白血病的治疗 • 以联合化疗为主 • 化学治疗使白血病的完全缓解率和5年无病生存率达到一定水平(70% 、40% ) • 异基因造血干细胞移植可使半数患者获得治愈。 • 早幼粒细胞白血病为一特殊亚型,可以应用诱导分化和促进凋亡的药物(维甲酸、三氧化二砷)治疗,效果满意。
慢性白血病的治疗 • 化疗效果不满意,无法根治。 • 针对其融合基因的靶向药物“伊马替尼”大大延长了慢性髓细胞白血病患者的无病生存期, • 单克隆抗体也提高了慢性淋巴细胞白血病的疗效。
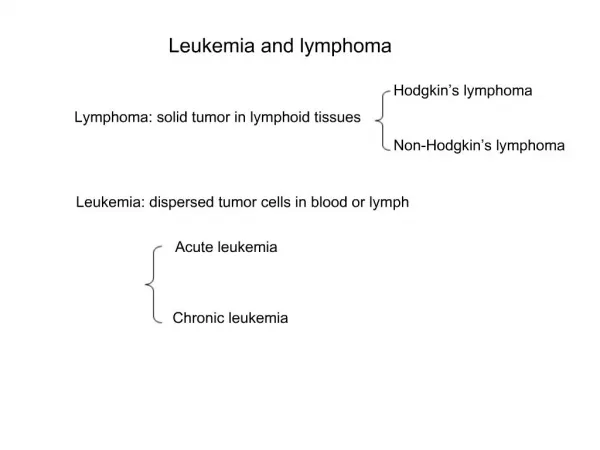
Lymphoma (淋巴瘤) • 淋巴瘤是血液系统也是免疫系统的恶性肿瘤。由于淋巴组织遍布全身,故淋巴瘤可以发生在身体的任何部位。淋巴结、扁桃体、脾及骨髓是最易受到累及的部位。通过组织病理学检查可以将淋巴瘤分为: • - Hodgkin lymphoma(霍奇金淋巴瘤) • - Non-Hodgkin lymphoma(非霍奇金淋巴瘤)
淋巴瘤的治疗 • 化疗、放疗、免疫治疗和手术切除。 • 可单独进行,也可采取联合措施,要根据疾病类型、存在的预后因素、患者的身体状况、经济条件而定。 • 霍奇金淋巴瘤疗效好,大多数可以治愈。 • 非霍奇金淋巴瘤有50余种病理亚型,疗效大不相同,自体造血干细胞移植约使40% 患者治愈。
多发性骨髓瘤(Multiple myeloma harmartoma,MMH ) • 多发性骨髓瘤是恶性浆细胞肿瘤。 • 浆细胞来自B淋巴细胞,能够分泌各种免疫球蛋白 • 骨髓瘤细胞也可分泌某一种免疫球蛋白或轻链,但是单克隆性。 • 此病多发生于中、老年人,主要症状为骨痛、多发骨折,往往有贫血和肾功能不全、血沉增快、球蛋白增多、尿蛋白阳性等,都是本病的诊断线索。 • 骨髓检查发现骨髓瘤细胞、血液中单克隆免疫球蛋白增高或尿液中有单克隆轻链和骨骼有溶骨眭损害,这是多发性骨髓瘤的诊断依据。
多发性骨髓瘤的治疗 • 以化疗和大剂量糖皮质激素为主,可缓解症状,但无法延长生存期。 • 近年采用沙利度安、雷那度安等血管新生抑制剂和蛋白酶体抑制剂硼替佐米等新药,疗效仅稍有改进。 • 60岁以下的较年轻患者可实行自体或异基因造血干细胞移植,有望延长生存期。
Mechanisms of antineoplastic drugs 细胞毒类抗肿瘤药物(Cytotoxic agents): • Interrupt the biosynthesis of nucleic acids • Interrupt the structure and functions of DNA • Interrupt transcription and synthesis of RNA • Inhibit the synthesis and functions of proteins 非细胞毒类抗肿瘤药物(Non-cytotoxic agents): • Regulate hormone levels • Molecular targeting agents • Others
Classification of Cytotoxic agents • 细胞周期特异性药物(Cell cycle specific agents, CCSA) - generally most effective in hematologic malignancies and in solid tumors in which a relatively large proportion of the cells are proliferating or are in the growth fraction. • 细胞周期非特异性药物(Cell cycle non-specific agents,CCNSA) - particularly useful in low growth fraction solid tumors as well as in high growth fraction tumors
作用机理 • 影响核酸(DNA、RNA)生物合成的药物 • 二氢叶酸还原酶抑制剂—甲氨蝶呤MTX--ALL • 嘌呤核苷酸类似物—巯嘌呤(6-MP)--ALL • 核苷酸还原酶抑制剂--羟基脲(HU)--CML • DNA多聚酶抑制剂 --阿糖胞苷(Ara-C)--AML • 直接破坏DNA并阻止其复制的药物 • 烷化剂— • 氮芥—HL ,NHL • 环磷酰胺(CTX)--ALL,MMH多发性骨髓廇 • 马利兰(白消安,Busulfan)--CML • 卡莫司汀(BCNU)--NHL、骨髓廇 • 抗生素类 • 丝裂霉素(MMC)--CML、NHL • 博莱霉素(BLM)--淋巴瘤联合治疗 • 拓扑异构酶抑制剂: • 喜树碱(CPT)--AML、CML • 鬼臼毒素--依托泊甙 (Etoposid, VP-16) –恶性淋巴廇
干扰RNA合成的药物 • 放线菌素D(DACT)--HL、NHL、 • 多柔比星(阿霉素,ADM)--ALL、AML • 柔红霉素(DRN)--ALL、AML • 影响蛋白质合成的药物 • 微管蛋白活性抑制剂 • 长春碱类 —ALL • 干扰核蛋白体功能的药物 • 三尖杉酯碱—AML、CML、NHL • 影响氨基酸供应的药物 • L-门冬酰胺酶(L-ASP)--ALL
非细胞毒类抗肿瘤药 • 调节体内激素水平的药物 • 糖皮质激素(glucocorticoids)--ALL,CLL,HL,NHL • Perdnisone • predinisolone • 分子靶向药物 • 酪氨酸激酶抑制剂:伊马替尼(imatinib,格列卫)--CML • 法尼基转移酶(FTase)抑制剂--AML • 促凋亡药物:Bcl一2抑制剂—ALL、AML • 单克隆抗体:利妥昔单抗(rituximab,美罗华)--治疗成人B细胞性非霍奇金淋巴瘤疗效显著
酪氨酸激酶抑制剂 • 目前研究较多的为C-Kit抑制剂和FLT3抑制剂。 • 伊马替尼是c-Kit抑制剂,其作用靶点为Bcr-Abl融合基因产物P210蛋白。 • Ph染色体阳性是成人CML 中最常见的细胞遗传学异常,约占20% ~30%,常规治疗效果差。 • 伊马替尼的应用改变了Ph+CML患者的预后。
Drugs for ALL • Drugs for remission induction (诱导缓解) • 长春新碱(Vincristine, VCR) • 泼尼松(Prednisone,P) • 柔红霉素(Daunorubicin, DNR); • 阿霉素(Adriamycin, ADM); • L-门冬酰胺酶(L-asparaginase, L-ASP); • 环磷酰胺(Cyclophosphamide, CTX); • 阿糖胞苷(Cytarabine, Ara-C); • 甲氨蝶呤(Methotrexate, MTX) • Drugs for consolidation(强化) • L-门冬酰胺酶(L-asparaginase, L-ASP) • 甲氨蝶呤 (Methotrexate, MTX) • 长春新碱(Vincristine, VCR) • 环磷酰胺(Cyclophosphamide, CTX);
Drugs for ALL • Drugs for maintenance(维持) • 巯嘌呤(6-MP) • 甲氨蝶呤(Methotrexate, MTX) • 长春新碱(Vincristine, VCR) • corticosteroids • Drugs for CNSL • 甲氨蝶呤(Methotrexate, MTX) • hydrocortisone, • 阿糖胞苷(Cytarabine, Ara-C);
Drugs for AML • Drugs for remission induction(诱导缓解) • 柔红霉素(Daunorubicin, DNR) • 阿糖胞苷(Cytarabine, Ara-C); • 依托泊苷(Etoposide, VP16) • 急性早幼粒细胞白血病(M3,APL) • 全反式维甲酸(All trans retinoic acid, ATRA); • 三氧化二砷 (As2O3) • 丹参酮ⅡA(TanⅡA) • 抗CD33单抗: 应用最广泛的是Gemtuzumab ozogamicin(GO,Mylotarg;之前曾被成为CMA-676)。GO由美国Wyeth公司生产,是由人源化IsC_,4抗CD33单抗(取自哺乳动物的骨髓瘤细胞株)与一种细胞毒药物加利车霉素(calicheamicin)的衍生物相结合而成。 • Drugs for consolidation(强化) • 阿糖胞苷(Cytarabine, Ara-C); • 柔红霉素(Daunorubicin, DNR) • 6-MP • MTX
他,让白血病细胞“改邪归正” “癌症诱导分化技术”创始人、著名血液病学专家、中国工程院院士王振义教授 全反式维甲酸
New Drugs in AML • FLT3酪氨酸激酶抑制剂 • 法尼基转移酶抑制剂 • 转录调节剂(DNA去甲基药物和组蛋白去乙酰化酶抑制剂--地西他滨 • 多药耐药一1调节剂 • 目前主要有三代, 第一代调节剂包括奎宁和环孢素,疗效存在争议; • 第二代调节剂如Psc一833的III期试验表明缓解率低且毒性大。 • 第三代调节剂目前正在研究,包括Tariquidar、Zosuquidar等。 • BC L一2反义寡核苷酸(Oblimersen) • 抗血管生成药物 • 氯法拉滨(Clofarabine)是第二代核苷酸类似物,是一种核酸转化酶强抑制剂。
Drugs for CML • 羟基脲(Hydroxyurea, HU) • 马利兰(Busulfan, Bu) • 高三尖杉酯碱((homoharringtonine,HHT):治疗CML一线药 • Ara-C, • 6-MP, • CTX… • 甲磺酸伊马替尼(Imatinib mesylate, IM) • IFN
Drugs for CLL • 早期CLL的治疗 • 苯丁酸氮芥(Chlorambucil, CLB) • 晚期或进展期CLL的治疗 • 嘌呤类似物 • 氟达拉滨(Fludarabine, Flu) • 克拉屈滨(2-氯脱氧腺苷) • 皮质激素 • 单克隆抗体:美罗华 • 大剂量苯丁酸氮芥
Drugs for HL • 阿霉素 (ADM) • 博来霉素(Bleomycin, BLM) • 长春新碱 (Vincristine, VCR) 、长春瑞滨 • 依托泊苷、司莫司汀、中草药如灵芝等。
利妥昔单抗(rituximab,美罗华):1997年美国FDA 批准抗CD20单克隆抗体美罗华(Rituximab)上市是一个历史性的里程碑。 美罗华已经被欧盟批准联用化疗作为侵袭性和惰性型NHL的一线治疗,以及惰性型NHL的二线单药治疗;欧洲已经批准美罗华用于复发或顽固的非霍奇余淋巴瘤患者的维持治疗,并于2006年7月批准罗氏公司的美罗华用于复发性或顽固性的滤泡性NHL患者。 CTX ADM VCR P VP16 Drugs for NHL
Methotrexate (MTX,甲氨蝶呤 ) • Action mechanisms - cell cycle specific agent (s-phase) - inhibits dihydrofolate reductase (DHFR) - inhibits folic acid synthesis. Folic acid is needed for the de novo synthesis of the nucleoside thymidine dTMP, and purine base, required for DNA/RNA/protein synthesis
Methotrexate (MTX) • Clinical uses - AL, including CNSL - chorionic epithelioma (绒毛膜上皮癌) - rheumatoid arthritis, psoriasis, induced abortion • Drug interaction - NSAIDs - Penicillin
Methotrexate (MTX) • Toxicity - Bone marrow suppression: leukopenia - Nausea and vomiting - Sores in the mouth or the lips (ulcerative stomatitis) - Hair loss (from head and body). - Signs of infection/fever, chills, cough, sore throat - Bruising or bleeding, black, tar-like stools. - Red spots on skin, rash, itching • Leucovorin (甲酰四氢叶酸)
Methotrexate (MTX) • Tolerance - decreased drug transport - decreased polyglutamate formation - synthesis of increased levels of DHFR through gene Amplification - altered DHFR with reduced affinity for methotrexate.
Cyclophosphamide (CTX) • Action mechanisms - non cell cycle specific agent - alkylats guanine base of DNA • Clinical uses: wild spectrum - Lymphoma - AL - Lung cancer - Breast cancer - Ovarian cancer - Nephrotic syndrome, rheumatiod arthritis
醛磷酰胺 丙烯醛 4-羟基环磷酰胺 羧基磷酰胺 磷酰胺氮芥 4-酮基环磷酰胺
Cyclophosphamide (CTX) • Toxicity - Chemotherapy-induced nausea and vomiting (CINV) - Bone marrow suppression - Hair loss (alopecia ) - Hemorrhagic cystitis (Prevention: sodium 2-mercaptoethane sulfonate 巯乙磺酸钠 )
Adriamycin (ADM) • Action mechanisms - non cell cycle specific agent - intercalates directed toward the minor groove. It has the highest preference for two adjacent G/C base pairs flanked on the 5' side by an A/T base pair, thereby interfering transcription process and mRNA synthesis. - inhibits the activity of topoisomerase type II, breaks the genomic DNA (Idamycin, 去甲氧柔红霉素 )
Adriamycin (ADM) • Clinical uses: wild spectrum, especially for drug-resistant tumors - AL and blastic phase of CML - Lymphoma - Lung cancer - Breast cancer - Ovarian cancer - Stomach cancer - Bladder cancer - Liver cancer Should be only be administered in a rapid intravenous infusion (due to its low bioavailability).
Adriamycin (ADM) • Toxicity - Bone marrow suppression - Nausea and vomiting - Cardiotoxicity (Prevention: dexrazoxiane) - Hair loss - Darkening of the skin - Renal, hepatic and cardiac function should be monitored routinely.
Vincristine (VCR) • Action mechanisms - cell cycle specific agent (m-phase and G1-phase) - binds to tubulin dimers, inhibiting assembly of microtubule structures (spindle), thereby arrests mitosis in metaphase. - also interrupts RNA polymerase and protein synthesis (G1-phase)
Vincristine (VCR) • Clinical uses: - ALL (with prednisone) -Lymphoma (NHL, and less, HL) - Lung cancer - Nephroblastoma • Toxicity: - Peripheral neuropathy - Bone marrow suppression - Nausea and vomiting - Hair loss Should be only be administered by intravenous injection (due to its low bioavailability).
Cytarabine (Ara-C) • Action mechanisms - cell cycle specific agent (s-phase) - the derivative Ara-CTP inhibits DNA and RNA polymerase and nucleotide reductase enzymes needed for DNA synthesis, thereby interfering DNA chain elongation and repair. - Ara-CTP is incorporated directly into DNA and functions as a DNA terminator, interfering DNA chain elongation.
Cytarabine (Ara-C) • Clinical uses: mainly for hematologic cancers - AML (M3/M4/M5) - Lymphoma - ALL - CNSL Should be only be given by continuous intravenous infusion due to its fast inactivation.
Cytarabine (Ara-C) • Toxicity: - Bone marrow suppression (leukopenia, thrombocytopenia, anemia, megaloblastosis) - Anorexia (cerebellar toxicity), nausea, vomiting - Hepatic dysfunction - stomatitis (口腔炎), conjunctivitis (结膜炎), pneumonitis (肺炎), fever, and dermatitis (皮炎).
Mercaptopurine (6-MP) • Action mechanisms - cell cycle specific agent (in particular s-phase and also postpones G1-phase) - the derivative TIMP inhibits purine nucleotide synthesis and metabolism.
Mercaptopurine (6-MP) • Clinical uses: - ALL (for maintenance therapy, due to its slow action) - Pediatric NHL - polycythemia vera (红细胞增多症) - inflammatory bowel disease • Toxicity - myelosuppression - diarrhea, nausea, vomiting, loss of appetite, stomach/abdominal pain - mouth sores - bleeding - Allopurinol increases the toxicity of 6-MP.