Download
1 / 27
270 likes | 368 Views
Surveillance of Individuals At High Risk For Developing Pancreatic Cancer. Marco Bruno. Erasmus Medical Center, Rotterdam. Pancreatic Cancer Facts & figures. One of the most fatal malignancies Overall 5-year survival rates < 3% Median survival 6 months

E N D
Surveillance of Individuals At High Risk For Developing Pancreatic Cancer Marco Bruno Erasmus Medical Center, Rotterdam
Pancreatic Cancer Facts & figures • One of the most fatal malignancies • Overall 5-year survival rates < 3% • Median survival 6 months • Irresectable at diagnosis due to late, non-specific symptoms and high metastatic potential • Poor response to chemo- and radiotherapy • Poor 5 year survival rates, even after potentially curative surgical resection
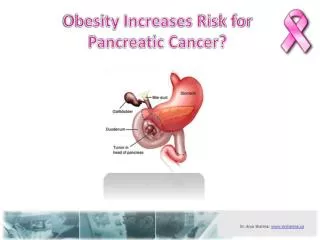
Pancreatic Cancer Environmental factors • Main risk factor: cigarette smoking • 2- to 3-fold elevated risk • accounts for 25% all cases • dose-response relationship • ↓ age of onset • Less well established: • fat, meat, salt • exposure to certain chemicals • diabetes mellitus, obesity • Possibly protective: fresh fruits and vegetables, dietary fiber, vitamin C
Hereditary Pancreatic Cancer Genetic factors I In about 10 to 15% of pancreatic cancers genetic factors seem to play a prominent role
Hereditary Pancreatic Cancer Genetic factors II • Inherited (tumor) syndromes which predispose to pancreatic cancer (syndromal) • (FAMMM,HBOC, HNPCC or Lynch syndrome, Peutz-Jeghers syndrome, ataxia-teleangiectasia, FAP, Li-Fraumeni syndrome) • Hereditary pancreatitis (trypsinogen mutations) • Accumulation of pancreatic cancer within a family without a known mutation
Hereditary Pancreatic Cancer Genetic factors III
Familial Pancreatic Cancer Without a known mutation • Autosomal dominant inheritance • Variable penetrance • No known susceptibility genes • Risk of pancreatic cancer increases with an increasing number of affected members: RR reaching a maximum of 57-fold in ≥ 3 affected family members • Cancerous genotype: • penetrance of the gene • environmental factors
Surveillance in Hereditary Pancreatic Cancer Ultimate goal Prevention of early death by: Detection of a precursor lesion before progression towards invasive carcinoma or Detection of an ‘early’ asymptomatic potentially curable malignancy
Pancreatic Cancer (Benign) precursor lesions • Stepwise, cumulative pathogenesis; activation K-ras, over-expression Her-2/neu (early), inactivation p16 and p53 (later) • Adenoma-carcinoma like sequence with curable, non-invasive precursor lesions: PanIN I-III, IPMN (SB – MB type)
Carcinogenesis Genetic model adapted from Fearon and Vogelstein
Pancreatic Intrapithelial Neoplasia Stages PanIn-1A to PanIn-2 • Wendt et al. 2007
Pancreatic Intrapithelial Neoplasia Stages PanIn-2 to PanIn-3 • Wendt et al. 2007
Pancreatic Cancer (Benign) precursor lesions • Stepwise, cumulative pathogenesis; activation K-ras, over-expression Her-2/neu(early), inactivation p16 and p53 (later) • Adenoma-carcinoma like sequence with curable, non-invasive precursor lesions: PanIN I-III, IPMN (SB – MB type) • IntraPancreatic Mucinous Neoplasia (IPMN) • Unknown interval of progression to invasive carcinoma; between 1 and 10 years
Imaging in Pancreatic Cancer Potentially promising techniques • MRI • non-invasive • sensitivity 83-87%, specificity 81-100% for diagnosing pancreatic cancer • no radiation exposure • EUS • invasive • sensitivity 95%, specificity 80% for diagnosing pancreatic cancer • has the ability to identify early lesions • despite invasiveness, low risk for adverse effects • operator-dependent
Surveillance in HereditaryPancreatic Cancer Literature data • Prospective controlled study • 78 ‘high’ risk individuals • 6 peutz-Jeghers patients • 72 individuals with 3 or more affected relatives • not belonging to p16, herid pancreatitis or HNPCC families • 4 patients with known BRCA2 mutation • 31 suspected of possibly having BRCA2 mutation based on Ashkenazi Jewish ancestery • Yield: 8 patients with neoplastic lesion • benign IPMN (n=6) • malignant IPMN (n=1) • pancreatic intraepithelial neoplasia (n=1) Canto et al. Clin Gastroenterol 2006: 4; 766-81
Surveillance in HereditaryPancreatic Cancer Prospective study • Partnership between Erasmus MC, AMC, AvL, and UMCG • Design: multi-centre, prospective, cohort study • Aim: to evaluate the feasibility and effectiveness of surveillance for early pancreatic neoplasia in high-risk individuals • Methods: one-yearly repeated investigations with EUS and MRI
Surveillance in HereditaryPancreatic CancerInclusion criteria I • PC prone hereditary syndromes with a cumulative lifetime risk >10% • carriers of mutations in CDKN2A, PRSS1 and STK11 genes • patients with a clinical diagnosis of Peutz-Jeghers syndrome but without a known gene mutation • PC prone hereditary syndromes with an unknown cumulative lifetime risk, or <10% • carriers of a germline mutation in BRCA2, BRCA1, MLH1, MSH2, APC or p53 in families with PC • at any age in ≥ 2 relatives who are (proven, obligate or supposed) carriers of these mutations; • with at least one histologically confirmed PC
Surveillance in HereditaryPancreatic CancerInclusion criteria II • Familial pancreatic cancer (site-specific), i.e. • a. ≥ 2 first-degree relatives with PC or • b. ≥ 3 relatives of any degree with PC or • c. ≥ 2 relatives of any degree with PC, one of whom was aged 50 years or younger at the time of diagnosis; - with at least one histologically confirmed PC in all subcategories and without obvious relation to any currently recognized hereditary syndrome - screening of first degree relatives of family members with PC
Surveillance in HereditaryPancreatic Cancer Prospective study • Main outcome parameter: number (percentage) of patients in whom a pancreatic cancer or precursor lesions are detected • Secondary outcome parameters (among others) • comparison between yield EUS and MRI • inter-observer agreement (video recordings) • psychological burden of surveillance • (long-term) outcome of operated patients • In addition: yearly collection of blood and fecal samples for future biomarker studies
Surveillance in HereditaryPancreatic Cancer Prospective study: first results • 48 patients included (20 M / 28 F, 51 y 27-75) • First time surveillance of asymptomatic individuals • 14 FAMMM, 22 familial pancreatic cancer, 3 hereditary pancreatitis, 2 Peutz-Jeghers, 3 BRCA1 and 2 BRCA2 mutation carriers with familial clustering of PC, and 2 p53 mutation • Yield: • 3 patients (6%) with pancreatic masses (12, 27, 55 mm) • sidebranch IPMN-like lesions in 7 patients (15%) [precursor lesions??] Poley et al. AM J Gastroenterol 2009:104; 2175
Hereditary Pancreatic Cancer Study Case example I
Hereditary Pancreatic Cancer Study Case example II
Surveillance in HereditaryPancreatic Cancer Ongoing study; interesting observations I • n=82 • 46% male, median age 51y (SD 9.6) • 47.6% FPC, 26.8% p16-Leiden, 14.6% BRCA2, 4.9% BRCA1, 3.7% PJS, 2.4% p53 • Focal lesions detected n=29 (45.4%) • mass n=3 (3.7%) • cyst n=20 (24.7%) • focal area of hypoechogenicity n=6 (7.3%)
Surveillance in HereditaryPancreatic Cancer Ongoing study; interesting observations II • Interval-EUS was performed in all cases with a focal area of hypoechogenicity of undetermined significance • spontaneous disappearance n=4 • persistent lesion n=2 • In 3/4 cases FU EUS after 12 months confirmed the absence of the previously detected lesions. In 1/4 cases FU12 months investigations are still pending.
Surveillance in HereditaryPancreatic Cancer Psychological burden • For weeks after the intake surveillance investigations • Response rate of 83% • Main reasons to participate in program • chance of early detection and better treatment prospects (100%) • contribution to scientific research • Major concerns • chance that a relative develops cancer: 34% • often or almost always concerned about developing cancer themselves: 31% • 17% of respondents have clinically relevant levels of depression and/or anxiety
Surveillance in HereditaryPancreatic Cancer Conclusion & summary I • EUS and MR are promising techniques for surveillance being able to detect “precursor” lesions and/or small carcinoma’s • We are only at the beginning of exploring the possibilities and prospects of pancreatic cancer surveillance • By no means it has been proven yet that we are doing good for the individuals at this point in time • The only sensible thing to do is to do surveillance within well defined research protocols and learn from its results
Surveillance in HereditaryPancreatic Cancer Conclusion & summary II • Many questions remain: • more accurate risk assessment of pancreatic cancer in various syndromes? • which individuals should be surveyed? • what is the most optimal (and feasible) surveillance interval? • is a non-invasive diagnostic modality (MRI) equally effective in detecting these early lesions? • at which time should a resection be performed? • is a total pancreatectomy indicated? • does early detection change the course of the disease; do patients survive and is mortality actually lowered?