Inhibitors
Inhibitors. Why they happen What are they How to control them Treatment options. Why Inhibitors H appen. Genetics Hemophilia severity More common in severe hemophilia FVIII mutations Mutations in intron 22 and 1 (regions inside a gene) Nonsense mutations Stop codon

Inhibitors
E N D
Presentation Transcript
Inhibitors Why they happen What are they How to control them Treatment options
Why Inhibitors Happen • Genetics • Hemophilia severity • More common in severe hemophilia • FVIII mutations • Mutations in intron 22 and 1 (regions inside a gene) • Nonsense mutations • Stop codon • Inversion mutations • DNA is reversed in (breaks off DNA and reinserts in reverse) • Family History • Higher chance of family member developing inhibitor if in family • Race/Ethnicity • Subtypes of FVIII (different types in different race/ethnicity, rFVIII is based on white FVIII) 3X higher
Environmental • Environmental • Intensive FVIII exposure • Continuous infusions • surgery --Immunological/inflammatory/infectious events Stimulation of immune system to produce antibodies • Use of rFVIII products • 27% in PUPs (Previously Untreated Patients)
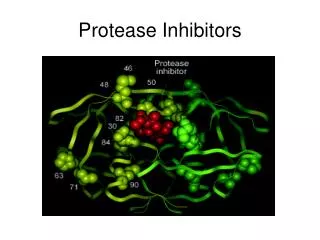
Types of Inhibitors • Hemophilia A and B inhibitors • FVIII • FIX • Acquired Hemophilia • The body's natural clotting process is disrupted • The body produces antibodies that fight its own blood-clotting proteins (auto-immune) • Not genetic, no family history
What are Inhibitors • Epitopes • A binding site on the antigen • Inhibitors are antibodies • Antibodies are produced by your body in response to disease (viral or bacteria) • Antigen • Foreign object in body
Presentation of Inhibitor • Uncontrolled bleeding in patient • Patient is given factor with bleed • Bleeding is not controlled with factor Breakthrough bleeding on prophy --Signs of bleeding while on regular treatment of factor VIII or IX
Bethesda/Nijmegen Assay • Bethesda is the test performed to measure inhibitors • One BU is the amount of inhibitor needed to inactivate 50% of FVIII in pooled normal plasma • Nijmegen assay • Low level antibodies • Antibody/Elisa test • Short half life
Classifications of Inhibitors • Low titer • 5 BU or less • High titer • 5 BU or higher • Low-responding • Never rise above 5 BU (not anamnestic) • High-responding • Above 5 BU (sharp rise in antibody titer within 5-6 days of fVIII exposure
Immune Tolerance Induction • Goal-To restore normal replacement of factor • BONN • High responding-FVIII 100-150 IU/KG every 12 hours • Van Creveld/Dutch Protocol • FVIII given 25IU/KG every other day • Malmo Protocol • BONN protocol with immunosuppressant w/corticosteroids and cyclophosphamide, IVIG
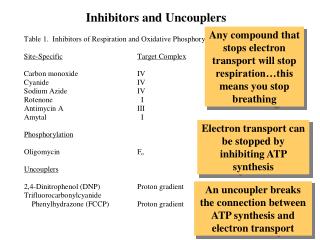
Treatment Options • NovoSeven • rFVIIa • Intrinsic pathway • Induces hemostasis by activating sufficient FX on activated platelet surface thrombin generation • Feiba • aPCC (prothrombin complex concentrate) • Promotes hemostasis by providing prothrombin (factor 2) and activated factor X (FX) converts prothrombin to thrombin (clot formation)
Conclusion • Inhibitors are the most serious complication in hemophilia • Researchers are looking at the time to start replacing clotting factor in PUPs • Family History • Use of other FVIII subtypes (human plasma, Europe)