Download
1 / 22
430 likes | 1.41k Views
ACE Inhibitors. ACE = Angiotensin I Converting Enzyme 10 ACE inhibitors available in US: benazepril, captopril, enalapril, fosinopril, lisinopril, moexipril, perindopril, quinapril, ramipril and trandolapril.

E N D
ACE Inhibitors • ACE = Angiotensin I Converting Enzyme • 10 ACE inhibitors available in US: • benazepril, captopril, enalapril, fosinopril, lisinopril, moexipril, perindopril, quinapril, ramipril and trandolapril. • ACE inhibitors were the 4th most prescribed drug class in the U.S (159.8 million Rx in 2008). • Lisinopril was the 2nd most prescribed drug in the US (75.5 million Rx in 2008).
The Renin-Angiotensin and Kallikrein-Kinin Systems From: Skidgel RA and Erdös EG, Hypertension Primer, 4th Edition, Chap. A15, 2008.
Peptide Hormone Processing and Drug Development Strategies Receptor 1 Prohormone Endoprotease Block Activity Processing Enzyme Enhance Activity Active Peptide Enhance Activity Peptidase 1 Peptidase 2 Receptor 2 Block Activity
ACE DISTRIBUTION • Widespread, concentrated on: • Endothelial surface of the vasculature • Epithelial Brush borders • Renal proximal tubules • Small intestine • Placenta • Choroid plexus ACE
Regulation of Renin Release: Renal Baroreceptor - senses pressure in wall of afferent arteriole; decrease stimulates renin secretion Macula Densa– senses chronic change in distal tubule salt delivery; decrease induces renin release. Sympathetic Nerves – JG cells are directly innervated by sympathetic nerves; stimulation increases renin secretion Angiotensin II- stimulates AT1 receptors on JG cells to decrease renin release
ACE Inhibitors ACE AT1 Receptor Vasoconstriction Aldosterone release Na+ Retention Pro-inflammatory Oxidative stress Proliferation of Sm. muscle/myocytes Blood Pressure Mechanism of Action of ACE Inhibitors Liver Angiotensinogen Kininogen Renin Kallikrein Kinin B2 Receptor Bradykinin Angiotensin I (Inactive) Chymase Cathepsin G Angiotensin II Vasodilation Na+ Excretion Bradykinin(1-7) (Inactive)
ACE Mechanism of Action of ACE Inhibitors II Angiotensinogen ACE Inhibitors Renin Endopeptidases AT1-7/Mas Receptor Angiotensin 1-7 Angiotensin I (Inactive) Vasodilation Na+ Excretion Anti-inflammatory Oxidative stress Angiotensin II Angiotensin 1-5 (Inactive) AT1 Receptor Vasoconstriction Aldosterone release Na+ Retention Pro-inflammatory Oxidative stress Proliferation of Sm. muscle/myocytes Blood Pressure
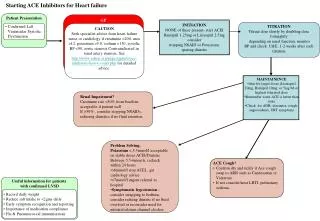
Clinical Use of ACE Inhibitors • Antihypertensive • ~ 50% response (~90% with diuretic) • ↓Systemic Vascular Resistance • ↓Stress or Relfex induced sympathetic stimulation • → Heart rate • ↑ Sodium excretion, ↓ Blood volume • Congestive Heart Failure • ↓Vascular Resistance, Blood volume, Heart rate • ↑ C.O. (no change in myocardial O2 consumption) • Diabetic Nephropathy • Dilates afferent and efferent renal arterioles • ↓Glomerular capillary pressure • ↓Growth of mesangial cells/matrix due to Ang II?
Side Effects/Contraindications • Common • Dry Cough • 5 – 20% of patients • Not dose-related; occurs within 1 wk. – 6 mo. • Women > men • May Require cessation of therapy • Fetopathic Potential • Not teratogenic in 1st trimester • Developmental defects in 2nd or 3rd trimester • Rare • Angioneurotic Edema (or Angioedema) • ~0.1 - 0.5% of patients • Not dose-related; occurs within 1st week • Severe swelling of mouth, tongue, lips, airway • may be life-threatening
Side Effects/Contraindications • Rare • Hypotension • First dose effect in patients with elevated PRA, salt depletion, CHF • Hyperkalemia • In patients with renal insufficiency, diabetic nephropathy • Acute Renal Failure • Patients with renal stenosis, heart failure, volume depleted • Skin Rash • Extremely Rare (reversible) • Alteration/loss of taste • Neutropenia • Glycosuria • Hepatotoxicity
Drug Interactions • Antacids • May reduce bioavailability of ACE inhibitors • Capsaicin • May worsen ACE inhibitor-induced cough • NSAIDs • May reduce antihypertensive response to ACE inhibitors • K+-sparing Diuretics or K+ supplements • May exacerbate ACE inhibitor-induced hyperkalemia
Additional Beneficial Effects of ACE Inhibitors • Cardioprotective • Reduce incidence of second heart attack • Reduce cardiovascular complications in patients with risk factors • Reduce incidence of diabetes in high risk patients • Reduce complications in diabetic patients
Angiotensin (AT1R) Receptor Blockers (“ARBs” or “sartans”) Angiotensinogen Renin B2 Receptor Angiotensin I (Inactive) Bradykinin(1-7) (Inactive) Chymase Cathepsin G ACE Angiotensin II ARBs Bradykinin AT2 Receptor AT1 Receptor AT1 Receptor Vasodilation Na+ Excretion Anti-inflammatory Anti-proliferative Vasoconstriction Aldosterone release Na+ Retention Pro-inflammatory Oxidative stress Proliferation of Sm. muscle/myocytes Blood Pressure
Clinical Use of Angiotensin Receptor Blockers • Effects are Similar to those of ACE inhibitors • FDA Approved for: • Hypertension • All ARBs • Congestive Heart Failure • Valsartan approved (second line therapy if ACE inhibitors not tolerated) • Diabetic Nephropathy • Irebesartan and Losartan (some believe superior to ACE inhibitors)
Side Effects/Contraindications • Better tolerated than ACE inhibitors • Much reduced risk of cough • >2-fold lower risk of Angioedema • Other side effects, including fetopathic potential, the same as for ACE inhibitors
Renin Inhibitor AT1 Receptor Vasoconstriction Aldosterone release Na+ Retention Pro-inflammatory Oxidative stress Proliferation of Sm. muscle/myocytes Angiotensinogen Kininogen Renin Inhibitor Aliskiren Kallikrein Renin B2 Receptor Bradykinin Angiotensin I (Inactive) Chymase Cathepsin G ACE Angiotensin II Vasodilation Na+ Excretion Bradykinin(1-7) (Inactive) AT1 Receptor Blood Pressure
Clinical Use of Aliskiren (Renin Inhibitor) • FDA Approved for Hypertension • Currently being tested for use in Congestive Heart Failure and Diabetic Nephropathy • Side Effects/Contraindications • Generally well tolerated • Teratogenic • Low risk of cough and angioedema • Most common side effects (<5%): • Gastrointestinal disturbance • Headache/dizziness • Hyperkalemia • Rash (rare)