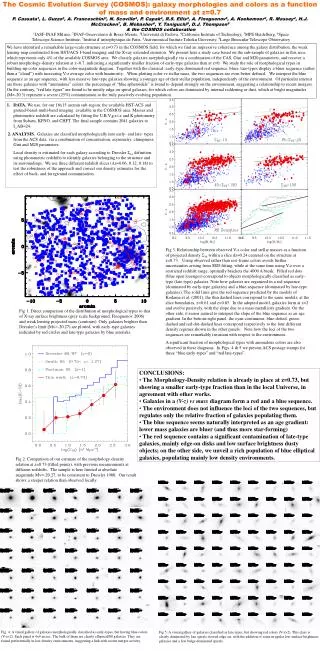
CONCLUSIONS
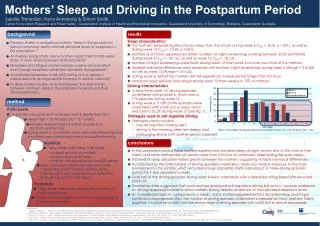
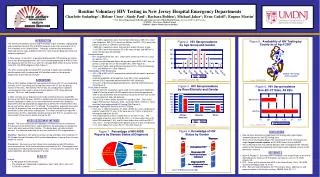
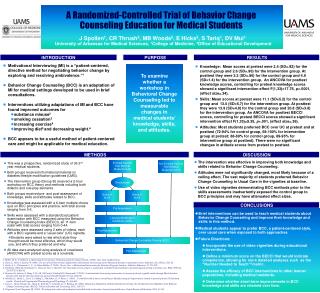
DISCUSSION. CONCLUSIONS. RESULTS. METHODS. INTRODUCTION. PURPOSE. Enrolled Second Year Medical Students N=36. Not Enrolled Second Year Medical Students N=110. Randomized. Group A N=18. Group B N=18. Pre Assessment. Lifestyle Modification Guidelines (LMG). Post Assessment.

CONCLUSIONS
E N D
Presentation Transcript
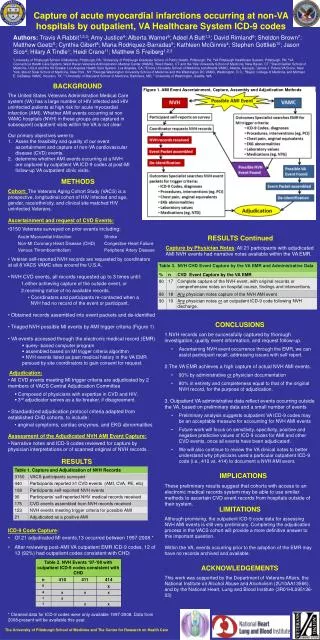
DISCUSSION CONCLUSIONS RESULTS METHODS INTRODUCTION PURPOSE Enrolled Second Year Medical Students N=36 Not Enrolled Second Year Medical Students N=110 Randomized Group A N=18 Group B N=18 Pre Assessment Lifestyle Modification Guidelines (LMG) Post Assessment Behavioral Change Counseling Training (BCC) Post Assessment A Randomized-Controlled Trial of Behavior Change Counseling Education for Medical Students J Spollen1, CR Thrush2, MB Woods2, E Hicks2, S Tariq1, DV Mui1 University of Arkansas for Medical Sciences, 1College of Medicine, 2Office of Educational Development • Motivational Interviewing (MI) is a “patient-centered, directive method for negotiating behavior change by exploring and resolving ambivalence.”1 • Behavior Change Counseling (BCC) is an adaptation of MI for medical settings developed to be used in brief consultations. • Interventions utilizing adaptations of MI and BCC have found improved outcomes for • substance misuse2 • smoking cessation3 • increasing exercise4 • improving diet5 and decreasing weight.6 • BCC appears to be a useful method of patient-centered care and might be applicable for medical education. • Knowledge: Mean scores at pretest were 2.4 (SD=.92) for the control group and 2.6 (SD=.96) for the intervention group. At posttest they were 3.2 (SD=.86) for the control group and 4.9 (SD=1.4) for the intervention group. An ANCOVA for posttest knowledge scores, controlling for pretest knowledge scores showed a significant intervention effect F(1,33)=17.76, p<.0001, (effect size=.34). • Skills: Mean scores at pretest were 11.1 (SD=5.2) for the control group and 13.0 (SD=5.7) for the intervention group. At posttest they were 13.9 (SD=4.8) for the control group and 20.8 (SD=3.8) for the intervention group.An ANCOVA for posttest BECCI scores, controlling for pretest BECCI scores showed a significant intervention effect F(1,33)=9.35, p<.001, (effect size=.36). • Attitudes: Most students preferred BCC over UC at pretest and at posttest (72-94% for control group, 68-100% for intervention group at pretest; 88-89% for control group, 89-95% for intervention group at posttest). There were no significant changes in attitude scores from pretest to posttest. To examine whether a workshop in Behavioral Change Counseling led to measurable changes in medical students’ knowledge, skills, and attitudes. • The intervention was effective in improving both knowledge and skills related to Behavior Change Counseling. • Attitudes were not significantly changed, most likely because of a ceiling effect. The vast majority of students preferred Behavior Change Counseling to Usual Care in the vignettes at baseline. • Use of video vignettes demonstrating BCC methods prior to the skills assessments inadvertently exposed the control group to BCC principles and may have attenuated effect sizes. • This was a prospective, randomized study of 36 2nd year medical students. • Both groups received informational material on diabetes lifestyle modification guidelines (LMG). • The intervention group (Group B) received a 2-hour workshop on BCC theory and methods including both didactic and role-play elements. • Both groups received pre- and post-assessment of knowledge, skills and attitudes related to BCC. • Knowledge was assessed with a 6-item multiple choice quiz on BCC principles and practice, with total scores ranging from 0-6. • Skills were assessed with a standardized patient examination with BCC measured using the Behavior Change Counseling Index (BECCI), an 11 item scale7with total scores ranging from 0-44. • Attitudes were assessed using 2 sets of videos, each with a BCC vignette and a “usual care” (UC) vignette. • Students were asked to rate which style they thought would be most effective, which they would use, and which they preferred and why. • All data were analyzed using analysis of covariance (ANCOVA) with pretest scores as a covariate. % • Brief interventions can be used to teach medical students about Behavior Change Counseling and improve their knowledge and skills in this method. • Medical students appear to prefer BCC, a patient-centered style, over usual care when exposed to both approaches. • Future Directions: • Incorporate the use of video vignettes during educational interventions. • Define a minimum score on the BECCI that would indicate competence, allowing for more detailed analyses such as the “Number Needed to Teach”8 metric. • Assess the efficacy of BCC interventions in other learner populations, including medical residents. • Determine whether short-term improvements in BCC knowledge and skills are retained over time. _________________________________________________________________________ 1. Miller, W. R., & Rollnick, S. Motivational interviewing: Preparing people for change (2nd ed.) (2002). New York: Guilford Press. 2. Dunn C, Deroo L, Rivara FP. (2001). The use of brief interventions adapted from motivational interviewing across behavioral domains: a systematic review. Addiction, Dec; 96(12):1725-42. 3. Stotts, A. L., Diclemente, C. C., & Dolan-Mullen, P. (2002). One-to-One - a Motivational Intervention for Resistant Pregnant Smokers. Addictive Behaviors, 27, 275-292. 4. Harland J, White M, Drinkwater C, Chinn D, Farr L, Howel D. The Newcastle exercise project: a randomised controlled trial of methods to promote physical activity in primary care. BMJ. 1999 Sep 25;319(7213):828-32. 5. Resnicow K, Jackson A, Wang T, De AK, McCarty F, Dudley WN, Baranowski T (2001). A motivational interviewing intervention to increase fruit and vegetable intake through Black churches: Results of the Eat for Life trial. American Journal of Public Health, 91 (10), 1686-93. 6. Woollard, J., Beilin, L., Lord, T., Puddey, I., MacAdam, D., & Rouse, I. (1995). A controlled trial of nurse counselling on lifestyle change for hypertensives treated in general practice: Preliminary results. Clinical and Experimental Pharmacology and Physiology, 22, 466-468. 7. Lane, C., Huws-Thomas, M., Hood, K., Rollnick, S., Edwards, K., & Robling, M. (2005). Measuring Adaptations of Motivational Interviewing: the Development and Validation of the Behavior Change Counseling Index (BECCI). Patient Education and Counseling, 56(2), 166-173. 8. Torgerson CJ and Torgerson DJ. (2003). The design and conduct of randomised controlled trials in education: Lessons from health care. Oxford Review of Education, 29(1), 67–80.