Download
1 / 24
260 likes | 542 Views
MONITORING DU NERF RECURRENT AU COURS DE LA CHIRURGIE THYROIDIENNE. Dr Eric Rondini-Gilli. Consultation d’ORL et de Chirurgie Cervico-Faciale, Pôle de santé du golfe de Saint-Tropez. UN SOUCIS CONSTANT : L’IDENTIFICATION ET LE RESPECT DU NERF RECURRENT.

E N D
MONITORING DU NERF RECURRENT AU COURS DE LA CHIRURGIE THYROIDIENNE Dr Eric Rondini-Gilli Consultation d’ORL et de Chirurgie Cervico-Faciale, Pôle de santé du golfe de Saint-Tropez
UN SOUCIS CONSTANT : L’IDENTIFICATION ET LE RESPECT DU NERF RECURRENT
UN SOUCIS CONSTANT : L’IDENTIFICATION ET LE RESPECT DU NERF RECURRENT • PARALYSIE RECURRENTIELLE • RARE ( 0,5 à 12 % ) • UNILATERALE >>> DYSPHONIE • BILATERALE >>> DYSPNEE
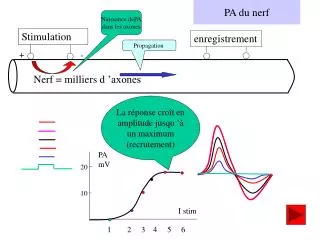
SURVEILLANCE ELECTROMYOGRAPHIQUE ET STIMULATION ELECTRIQUE • SONDE D’INTUBATION OROTRACHEALE EQUIPEE DE DEUX PAIRES D’ ELECTRODES
SURVEILLANCE ELECTROMYOGRAPHIQUE ET STIMULATION ELECTRIQUE • SONDE D’INTUBATION OROTRACHEALE EQUIPEE DE DEUX PAIRES D’ ELECTRODES • UNE SONDE DE STIMULATION
SURVEILLANCE ELECTROMYOGRAPHIQUE ET STIMULATION ELECTRIQUE • SONDE D’INTUBATION OROTRACHEALE EQUIPEE DE DEUX PAIRES D’ ELECTRODES • UNE SONDE DE STIMULATION • UN MONITEUR
EN PRATIQUE • CONTRE INDICATION DES CURARES • POSITIONNEMENT DE LA SONDE D’ INTUBATION • DIFFERENCE D’ IMPEDANCE, PÔLE TERRE, PÔLE +, STIMULATEUR AU PÔLE – • REGLAGES : INTENSITE DE STIMULATION 0,45 à 1 mA SEUIL DE DETECTION de 100 à 150 µV
Etude personnelle (Hôpital Beaujon/clinique chirurgicale de St-Tropez) • 163 patients vus pour pathologie thyroïdienne nodulaire entre 2001 et 2005. • 238 nerfs monitorés • 132 Femmes (81%) et 31 Hommes (19%) • Age moyen : 46 ans (18-78 ans) • Suivi moyen: 9 mois (1-74 mois)
2 % de la population adulte La plupart bénins Mais aucun argument certain sauf anapath définitive pour la bénignité Présomption de bénignité : <3cm, rond, souple, réguliers, non évolutifs, captant l’iode 123, hyperéchogènes, Inversement …
Type de Chirurgie Thyroïdectomie subtotale : 34 (21%) Lobo-isthmectomie : 88 (54%) Thyroïdectomie totale en un temps : 33 (20%) Thyroïdectomie totale en 2 temps : 8 (5%)
Signes cliniques • Nodule palpable : 104 patients (64%) • Goître palpable : 64 patients (40%) • Adénopathie palpable : 11 patients (7%) • Paralysie récurrentielle : 2 patients (1%)
Echographie • Echographiste entraîné, preciser le parenchyme, les aires ggaires • Nodules 123 (75%) • unique 77 (63 %) • multiples 46 (37%) • Taille du plus gros nodule • 29 ± 2,8 mm (8 mm 100 mm)
Cytoponction • Cytologiste / médecin entraîné, • Désormais de principe devant tout nodule significatif • Systematique pour tout nodule suspect, hypofixant, iso ou anechogène
Résultats post-opératoires Anatomopathologie • Lésions bénignes 134 (82%) • Lésions malignes 25 (18%) • - carcinomes papillaires 20 (12%) • - carcinomes vésiculaires 3 (2%) • - carcinome indifférencié 1 (1%) - adénocarcinome mucineux 1 (1%)
Complications post-opératoires • Cicatrices chéloïdes 4 (2%) • Hématomes de la loge thyroïdienne 4 (2%) • Paralysie récurrentielle unilatérale • - transitoire (1-12 mois) 2 (<2%) • définitive 1 (<1%) • Corrélation atteinte recurrentielle/seuils de stimulation perop • REPONSE A LA STIMULATION ELECTRIQUE de 0.5 à 1 mA • EN FIN D’ INTERVENTION, DANS TOUS LES CAS SAUF CINQ • Hypoparathyroïdie : • - transitoire (1-5 mois) 13 (8%) • - définitive 1 (1%)
Conclusions (1) • Taille moyenne des nodules de cette étude : 3 cm • 18 % de cancers (population hétérogène) • Pas de complications vitales, • Cytoponction si nodule isolé, unique, palpable et hypofixant en scintigraphie. • Chirurgie si nodule(s) plein(s) > 2 cm • L’amélioration de la sensibilité de la cytoponction doit permettre à terme de mieux sélectionner les indications chirurgicales. • Surveillance des nodules !
CONCLUSION Monitoring • AIDE AU REPERAGE ET A LA CONSERVATION DU NERF • VERIFICATION DE L’ INTEGRITE DU NERF EN FIN D’ INTERVENTION • CONFORT CHIRURGICAL (++) • DIMINUTION DE LA MORBIDITE • COÛT • INTERET MEDICO-LEGAL ?