Download
1 / 16
160 likes | 1.39k Views
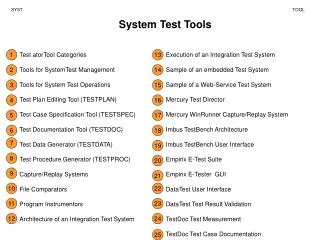
DRG and Code Reconciliation – CDI and HIM Coding Teamwork. Tessa Robinson, RN, BSN, CCDS CDI Supervisor, Nix Health Care System trobinson@nixhealth.com. Objectives. A. Define CDI-Coding reconciliation B. Review reconciliation process

E N D
DRG and Code Reconciliation – CDI and HIM Coding Teamwork Tessa Robinson, RN, BSN, CCDS CDI Supervisor, Nix Health Care System trobinson@nixhealth.com
Objectives • A. Define CDI-Coding reconciliation • B. Review reconciliation process • C. Coordinate learning opportunities • D. Identify root causes
What is CDI–HIM Coding Reconciliation • Reconciliation - the action of making one view or belief compatible with another. • For the CDI – Coding World, it’s the process of reviewing the medical record and comparing CDI findings to those in the Coding Summary, with adjustments as indicated so that the final DRGs are the same. • Goal: complete and accurate documentation and coding.
NIX Process CDI reviews and codes chart concurrently. CDI queries opportunities as identified. Final review is done at discharge prior to coding, for identification of any missed opportunities. Coding notified if missed opportunity is identified and will impact DRG. After discharge Coding reviews and codes chart.
Coding notifies CDI if any missed opportunity is encountered or if further clarification is needed for existing documentation. After chart is coded, CDI is notified of any mismatches. CDI does secondary review to identify cause of mismatch. CDI coding is either adjusted to match coder or mismatch is discussed between CDI and Coder. If unable to reconcile, account is referred to physician advisor or corporate HIM.
Collaboration • Identify educational opportunities • Education exchanges • Build and strengthen common goals • Hold regular joint meetings • Participate in joint professional events • Overcome challenges
Case # 1 History of presenting illness: The patient is a 67-year-old female with a past medical history of hypertension, diabetes, coronary artery disease, arthritis, CHF, and colon cancer status post colostomy placement. She presented with abdominal wound dehiscence that is leaking stool for the past week. Leakage has gradually and progressively worsened and it is foul smelling. Patient also noted to have acute renal failure with mild CHF exacerbation. Patient reported mild to moderate amount of pain increasing with activity, while decreased with rest and pain medications. Diagnosis: Possible colocutaneous fistula. Acute renal failure
Case # 1 con’t PROCEDURE PERFORMED: Revision of colostomy and drainage of abdominal wall abscess. PROCEDURE DIAGNOSIS: Dehiscence of ostomy with left abdominal and flank abscess Discharge Summary: During the hospital course, the patient was followed by Surgery. She underwent surgical intervention for repair of her enterocutaneous fistula and colostomy with drainage of abdominal wall abscess. Patient doing well, Acute on chronic systolic CHF improving, now tolerating PO, ARF resolved. Scheduled for discharge back to nursing home today.
Case # 1 con’t CDI Principle Diagnosis: Surgical wound dehiscence Other diagnosis: Acute on chronic systolic heart failure DRG 907 wt. 4.2161 Coding Principle Diagnosis: Colostomy complication Other diagnosis: Acute on chronic systolic heart failure DRG 344 wt. 2.9872 CDI-Coder discussion – agreement not reached. Case escalated to MD advisor and Corporate HIM Final DRG 907
Case # 2 HISTORY OF PRESENT ILLNESS: This patient is a 52-year-old male with a past medical history of diastolic congestive heart failure, diabetes type 2, hypertension, end-stage renal disease, currently receiving dialysis 3 times a week. The patient was directly admitted with concern for altered mental status due to progressive dementia versus acute encephalopathy. Patient has been having progressive memory loss and ability to perform ADLs over the past year. Diagnosis: Encephalopathy, concern for toxic metabolic causes. ESRD Diastolic heart failure HTN
Case # 2 con’t Discharge Summary: Patient admitted for Altered mental status, with chronic diastolic heart failure, ESRD, and hypertension. He was evaluated by Neurology and Psychiatry who at this time believe the patient most likely has early onset vascular dementia, with component of frontotemporal dementia given the patient’s acuity as well as clinical signs of irritability and personality changes. Patient to be discharged home with home health.
Case # 2 con’t CDI Principle Diagnosis: Vascular dementia Other Diagnosis: ESRD DRG 884 wt. 1.3479 Coding Principle Diagnosis: Other frontotemporal dementia Other Diagnosis: ESRD DRG 056 wt. 2.1245 CDI – Coder discussion. Coder dx has higher degree of specificity. Agreement reached. Result - CDI PDX change Final DRG 056
Case # 3 HISTORY OF PRESENT ILLNESS: The patient is a 63-year-old male with a past medical history of type 2 diabetes with polyneuropathy, quadriplegia, paroxysmal atrial fibrillation, COPD, asthma, neurogenic bowel, osteoarthritis, neurogenic bladder, recurrent urinary tract infections thought to be due to chronic indwelling catheter, dementia, and intellectual delay. There was concern for altered mental status and hypotension. He was admitted for septic shock and an infected sacral decubitus ulcer. DIAGNOSIS: Sepsis likely from UTI Septic shock Quadriplegia Sacral decubitus ulcer Hyponatremia Metabolic acidosis
Case # 3 con’t Discharge Summary: This is a 63-year-old male with a significant past medical history of type 2 diabetes with polyneuropathy, quadriplegia, paroxysmal atrial fibrillation, COPD, neurogenic bowel and bladder with chronic indwelling foley. The patient was found to be in septic shock on presentation. Blood and urine cultures were positive for E.coli. He has a stage 4 sacral decubitus ulcer which was treated by wound care nurse. Hyponatremia and acidosis resolved. Patient to discharge back to nursing home today.
Case # 3 con’t CDI Principle Diagnosis: Sepsis Other Diagnosis: Septic shock, quadriplegia, UTI, stage 4 decubitus ulcer DRG 871 wt. 1.8564 Coding Principle Diagnosis: Infection d/t indwelling catheter Other Diagnosis: ESRD DRG 698 wt. 1.6151 CDI – Coder discussion. PDX based on coding guidelines. Agreement reached. Result - CDI PDX change Final DRG 698
Documentation Grins • "History of sick as hell disease“ • Head CT shows no hemorrhoids! And, urine intake is low • "Eyes and nose continue to be within normal limits“ • "The chest xray has regrettably improved". • The lab test indicated abnormal lover function. • Discharge status: Alive but without permission. • Whilst in Casualty she was examined, Xrated and sent home.