TOXICOKINETICS
TOXICOKINETICS. Wongwiwat Tassaneeyakul Department of Toxicology Khon Kaen University. Toxicokinetics - the study of the time course of toxicant absorption, distribution, metabolism, and excretion How can we predict variability among individuals?

TOXICOKINETICS
E N D
Presentation Transcript
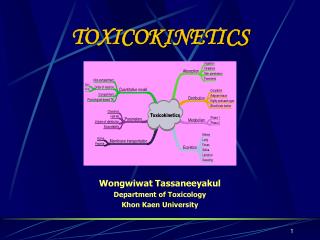
TOXICOKINETICS Wongwiwat Tassaneeyakul Department of Toxicology Khon Kaen University
Toxicokinetics- the study of the time course of toxicant absorption, distribution, metabolism, and excretion • How can we predict variability among individuals? • How can we extrapolate from animal models to humans? Site of action Plasma Conc. Dosage Exposure Toxic Effects Toxicokinetics Toxicodynamics
Toxicokinetic (TK) processes ABSORPTION DISTRIBUTION METABOLISM EXCRETION EXTERNAL BLOOD PLASMA PHASE-1 KIDNEYS MEMBRANE Oxidation LIVER BARRIERS xenobiotic lungs TISSUES saliva skin PHASE-2 pools sweat G.I. tract conjugation depots breast milk lungs sinks
Disposition of Xenobiotics absorption distribution excretion
Structural model of cell membrane • The ‘lipid sieve’ model explain how lipophilic small cpds can permeate through the membrane by passive diffusion • hydrophilic cpds cannot permeate unless there is a specific membrane transport channel or pump.
Mechanism of Membrane Permeation • Passive diffusion • Active transport • Facilitated transport • Pinocytosis
Transfer of Chemicals across Membranes • Passive transport determined by: - Permeability of surface - Concentration gradient - Surface area • Permeability depends on: For cell membranes: - Lipid solubility - pH of medium - pK of chemical For endothelium size, shape and charge of chemical PASSAGE ACROSS MEMBRANES Active Passive Facilitated
Uptake by Passive diffusion • Uncharged molecules may diffuse along conc. gradient until equilibrium is reached • No substrate specific • Small MW < 0.4 nm (e.g. CO, N20, HCN) can move through cell pores • Lipophilic chemicals may diffuse through the lipid bilayer
Uptake by Passive diffusion • First order rate diffusion, depends on • Concentration gradient • Surface area (alveoli 25 x body surface) • Thickness • Lipid solubility & ionization • Molecular size (membrane pore size = 4-40 A, allowing MW of 100-70,000 to pass through)
Weak Acids and Weak Bases HA <==> H+ + A- B + H+ <==> BH+ [ UI ] [ I ] [ UI ] [ I ] pKa = pH + log(HA/A-) pKa = pH+ log(BH+/B) pKa = 4.5 (a weak acid) pH = 2 pH = 7.4 0.1 = [ I ] [ I ] = 9990 100 = [ UI ] [ UI ] = 100 100.1 = total drug = 10090
Flicks’s law and Diffusion dD/dt = KA (Co - Ci) / t Where; dD/dt = rate of mass transfer across the membrane K = constant (coefficient of permeability) A = Cross sectional area of membrane exposed to the compound C0 = Concentration of the toxicant outside the membrane Ci = Concentration of the toxicant inside the membrane t = Thickness of the membrane
Facilitated Transport • Carried by trans-membrane carrier along concentration gradient • Energy independent • May enhance transport up to 50,000 folds • Example: Calmodulin for facilitated transport of Ca++
Active Transport • Independent of or against conc. gradient • Require energy • Substrate –specific • Rate limited by no. of carriers • Example: P-glycoprotein pump for xenobiotics (e.g. OC) • Ca-pump (Ca2+ -ATPase)
Uptake by Pinocytosis For large molecules ( ca 1 um) Outside: in-folding of cell membrane Inside: release of molecules Example: Airborne toxicants across alveoli cells Carrageenan across intestine
Rate of Absorption The rate of absorption determines the time of onset and the degree of acute toxicity. This is largely because time to peak (Tmax) and maximum concentration (Cmax) after each exposure depend on the rate of absorption. Rate the following processes in order of fastest to slowest: INTRAVENOUS> INHALATION >ORAL > DERMAL EXPOSURE.
Factors Affecting Absorption • Determinants of Passive Transfer (lipid solubility, pH, pK, area, concentration gradient). • Blood flow • Dissolution in the aqueous medium surrounding the absorbing surface.
Factors Affecting GI Absorption • Disintegration of dosage form and dissolution of particles • Chemical stability of chemical in gastric and intestinal juices and enzymes • Rate of gastric emptying • Motility and mixing in GI tract • Presence and type of food
Lungs Absorption • For gases, vapors and volatile liquids, aerosols and particles • In general: large surface area, thin barrier, high blood flow rapid absorption • Blood:air partition coefficient – influence of respiratory rate and blood flow • Blood:tissue partition coefficient
Lungs Absorption REMOVAL OF PARTICLES Absorption of Aerosols and Particles: 1- Particle Size 2- Water solubility of the chemical present in the aerosol or particle Lymph Physical Phagocytosis
Airway anatomy bronchial tree trachea • diffusion distance: ~20 mm • total exchange gas exchange area: ~80 m2
Airway anatomy alveoli trachea capillaries bronchial tree • diffusion distance blood/air: ~20 mm • total exchange gas exchange area: ~80 m2
Absorption Area in the Respiratory System Nasopharynge 5-30 µm Trachea Bronchi Bronchioles 1-5 µm Alveolar Region 1 µm
Skin Absorption • Must cross several cell layers (stratum corneum, epidermis, dermis) to reach blood vessels. • Factors important here are: lipid solubility hydration of skin site (e.g. sole of feet vs. scrotum)
Other Routes of Exposure • Intraperitoneal large surface area, vascularized, first pass effect. • Intramuscular, subcutaneous, intradermal: absorption through endothelial pores into the circulation; blood flow is most important + other factors • Intravenous
Bioavailability Definition: the fraction of the administered dose reaching the systemic circulation for i.v.: 100% for non i.v.: ranges from 0 to 100% e.g. lidocaine bioavailability 35% due to destruction in gastric acid and liver metabolism First Pass Effect
Systemic circulation Liver vein Liver Liver artery Vena portae and tributaries
FIRST PASS EFFECT Intestinal vs. gastric absorption Wilkinson, NEJM 2005
Extent of Absorption or Bioavailability Destroyed in gut Not absorbed Destroyed by gut wall Destroyed by liver Dose to systemic circulation
Bioavailability (F) Plasma concentration (AUC)o (AUC)iv i.v. route oral route Time (hours)
Principle For xenobiotics taken by routes other than the iv, the extent of absorption and the bioavailability must be understood in order to determine whether a certain exposure dose will induce toxic effects or not. It will also explain why the same dose may cause toxicity by one route but not the other.
Distribution • Distribution is second phase of TK process • defines where in the body a xenobiotic will go after absorption • Perfusion-limited tissue distribution • perfusion ratedefines rate of blood flow to organs • highly perfused tissues (often more vulnerable) • liver, kidneys, lung, brain • poorly perfused tissues (often less vulnerable) • skin, fat, connective tissues, bone, muscle (variable)
Distribution into body compartments • Plasma 3.5 liters. (heparin, plasma expanders) • Extracellular fluid 14 liters. • (tubocurarine, charged polar compounds) • Total body water 40 liters. (ethanol) • Transcellular small.CSF, eye, fetus (must pass tight junctions)
Distribution • Rapid process relative to absorption and elimination • Extent depends on - blood flow - size, M.W. of molecule - lipid solubility and ionization - plasma protein binding - tissue binding
Distribution • Initial and later phases: initial determined by blood flow later determined by tissue affinity • Examples of tissues that store chemicals: fat for highly lipid soluble compounds bone for lead
Alter plasma binding of chemicals 1000 molecules 90.0 99.9 % bound 1 100 molecules free 100-fold increase in free pharmacologically active concentration at site of action. NON-TOXIC TOXIC
volume of distribution Chemicals appear to distribute in the body as if it were a single compartment. The magnitude of the chemical’s distribution is given by the apparent volume of distribution (Vd).
Volume of Distribution (Vd) Volume into which a drug appears to distribute with a concentration equal to its plasma concentration Amount of drug in body Vd = Concentration in Plasma
Vd can be calculated after an IV dose of a substance that exhibits "one-compartment model" characteristics. Vd = Dose / Initial Conc
Drug L/Kg L/70 kg Sulfisoxazole 0.16 11.2 Phenytoin 0.63 44.1 Phenobarbital 0.55 38.5 Diazepam 2.4 168 Digoxin 7 490 Examples of apparent Vd’s for some drugs
Competition-displacement between xenobiotics low bioavailability high bioavailability tolbutamide + warfarin (antocoagulant) tolbutamide (hypoglycemic drug)
Distribution • Blood Brain Barrier – characteristics: 1. No pores in endothelial membrane 2. Transporter in endothelial cells 3. Glial cells surround endothelial cells 4. Less protein concentration in interstitial fluid • Passage across Placenta
Free-plasma and erythrocyte-bound xenobioticsexample: lead binding to ALAD protein plasma Pb++ Blood Pb++ erythrocyte Pb++
CNS (brain) spongy bone kidney lower neurotoxicity higher renal toxicity lower plasma Pb++ - - higher erythrocyte Pb++ elevated blood Pb++ ALAD-2 polymorphism Free-plasma and erythrocyte-bound xenobioticsexample: lead binding to ALAD protein CNS (brain) spongy bone kidney higher neurotoxicity avg plasma Pb++ avg erythrocyte Pb++ average blood Pb++ ALAD-1 polymorphism
Normal blood capillaries • most capillaries are fenestrated • small gaps in capillary wallnot tightly sealed • allows paracellular permeation of small plasma solutes • hydrophiles can pass thru capillary wall into tissue ECF • must be smaller than 100 A • lipophiles cannot easily permeate capillary wall by paracellular permeation • mostly bound to plasma proteins • permeate capillary wall by passive diffusion in free plasma phase
Brain capillaries: blood-brain barrier (BBB) brain capillaries are unfenestrated -- no gaps cell membrane of capillary endothelium cells sealed shut tight intercellular junctions constitute the blood brain barrier (BBB) paracellularpermeation of plasma solutes is impossible hydrophiles dissolved in blood typically cannot pass through the BBB into brain lipophiles can easily permeate the BBB by transcellular permeation (passive diffusion)
Endothelial cell Tight junction Basal membrane (porous) Astrocyte Capillary structure General circulation Central nervous system: ‘blood brain barrier’
Elimination • Includes all mechanisms for removing xenobiotics from the body • Kel is the elimination rate constant • One compartment model • Slope = -kel/2.3 • Two Compartment model • = distribution Constant • slope = ß/-2.3 and is the elimination rate constant • Is calculated after pseudoequilibrium has been established
Clearance (CL) Defined rate xenobiotic eliminated from the body • Can be defined for various organs in the body • Sum of all routes of elimination • CLtotal = CLliver + CLkidney + CLintestine