Download
1 / 51
510 likes | 683 Views
Management of HBV Infection. 28 year old woman with no significant PMH is referred for evaluation of HBsAg positivity She is fit and healthy and asymptomatic She was born in Korea and her family moved to the UK when she was 5 yo She works in advertising, is single, and has no children.

E N D
28 year old woman with no significant PMH is referred for evaluation of HBsAg positivity She is fit and healthy and asymptomatic She was born in Korea and her family moved to the UK when she was 5 yo She works in advertising, is single, and has no children. She is sexually active with one male partner and does not use barrier contraception. She drinks approximately 15 units of alcohol/ week Non smoker She also denies a history of blood transfusion or intravenous-drug use. Her mother was diagnosed with hepatitis B and HCC 8 months ago. She has no siblings
OE No stigmata of CLD Abdomen: soft, non-distended, non-tender, liver edge smooth, liver span 8 cm by percussion, no splenomegaly Bloods HBsAg: positive HIV: negativeHepatitis C virus (HCV) antibody (Ab): negativeHepatitis A virus (HAV) IgG/IgM: negative ALT 38 U/L (10-50 U/L) FBC NormalAST 26 U/L (10-40 U/L) U&E NormalALP 114 U/L (30-140 U/L) INR NormalBili 17 mol/L (10-23)
Which of the following blood tests would provide the most useful information • to characterize the status of chronic hepatitis B and guide recommendations • regarding antiviral therapy? • HBeAg, HBsAb, and hepatitis B core antibody (HBcAb) • HBeAg, HBeAb, and HBV genotype • HBeAg, HBeAb, and HBV DNA viral load • HBeAg, HBV DNA, and sequencing for YMDD mutation
Which of the following blood tests would provide the most useful information • to characterize the status of chronic hepatitis B and guide recommendations • regarding antiviral therapy? • HBeAg, HBsAb, and hepatitis B core antibody (HBcAb) • HBeAg, HBeAb, and HBV genotype • HBeAg, HBeAb, and HBV DNA viral load • HBeAg, HBV DNA, and sequencing for YMDD mutation
HBV DNA HBV DNA load is measured by polymerase chain reaction (PCR) This can be qualitative or quantitative In a prospective cohort study of >3500 patients with chronic hepatitis B, serum HBV DNA level was shown to be a powerful predictor progression to cirrhosis HBV DNA levels tend to be higher in HBeAg-positive patients compared with HBeAg-negative patients.
.4 Baseline HBV DNA Level, copies/mL .3 Cumulative Incidence of Liver CirrhosisREVEAL HBV Study 37.1% 1.0 x 106 n=627 1.0-9.9x105 n=344 1.0-9.9x104 n=649 300-9.9x103 n=1210 <300 n=944 n=3,774 23.0% Cumulative incidence of liver cirrhosis .2 .1 10.0% 6.3% 5.2% 0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 Year of follow-up P value for log-rank test, <0.001 Uchenna H. I, et al. Gastroenterology 2006; 130:678-686
High Serum HBV DNA Levels are Associated with Increased Risk of HCC Mortality HBV DNA Negative HBV DNA Low < 105copies/mL RR = 1.7 (0.5-5.7) HBV DNA High > 105copies/mL RR = 11.2 (3.6-35.0) p< 0.001 across viral categories Chen G, et al. J Hepatology 2005; 42 (suppl 2):477A. Chen G, et al. Hepatology 2005; 40 (suppl 1):594A.
Genotype There are 8 genotypes of hepatitis B (A through H) The clinical utility of HBV genotype has not yet been clearly defined. Although it is not routine, it may be reasonable to document HBV genotype prior to commencing antiviral therapy as in future HBV genotype may assumea more pivotal role in the management of hepatitis B.
The Emerging Role of HBV Genotypes Clear association with: Precore/core promoter mutations Rates of HBeAg clearance Development of HBeAg-neg Chronic Hepatitis B Possible association with: Liver disease activity Progression to cirrhosis Risk of HCC Response to IFN and nucleoti(si)de analogs
HBV Genotypes F D A A B C D C Bj D D C D D Ba E F F A Fung & Lok, Hepatology 2004;40:790-2
Further Blood results AST 35 U/L HBsAg: positiveALT 40 U/L HAV IgG/IgM: negative bilirubin 20 mmol/L HCV Ab: negative ALP 121 mg/d Hepatitis D virus (HDV) IgM: negativeHIV: negative HBeAg: negativeHBeAb: positiveHBV DNA: 25,000 IU/mLHBV genotype: B
Which statement is false regarding this patient's hepatitis B status? • She is an inactive carrier of hepatitis B • She is not in the immune-tolerant phase • She likely has a mutation in the precore or core promoter region • of the HBV genome • HBeAg positivity is associated with a better prognosis than • HBeAg negativity
Which statement is false regarding this patient's hepatitis B status? • She is an inactive carrier of hepatitis B • She is not in the immune-tolerant phase • She likely has a mutation in the precore or core promoter region • of the HBV genome • HBeAg positivity is associated with a better prognosis than • HBeAg negativity
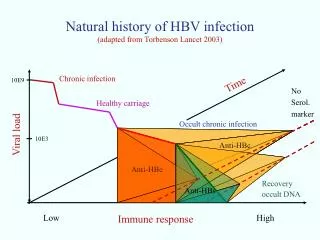
HBeAg Anti-HBe HBV-DNA ALT immunetolerance immuneclearance inactivecarrier reactivation Viral fluctuation patterns are different in different stages of the disease
Serologic Markers of Hepatitis B HBV Status HBsAg positive > 6 months Chronic hepatitis B Anti-HBs positive Immunity to HBV infection (vaccination or clearance of infection)* Anti-HBc IgG positive Prior exposure to HBV Anti-HBc IgM positive Acute HBV infection or reactivation of HBV HBeAg positive Active viral replication HBeAg negative Pre-core/core promoter mutation or non-replicative HBV infection Anti-HBe positive HBeAg seroconversion or precore/core promoter mutation
Which of the following statements is true regarding lifestyle modifications and prevention of spread of infection in this patient? A)The amount of alcohol that this patient consumes is insufficient to have an adverse impact on disease course B) Her sexual partner is at high risk for acquiring HBV infection, and therefore should be started on hepatitis B immune globulin (HBIG) C) The patient should receive a 2-dose series of vaccinations for hepatitis A D) The risk for sexual transmission of hepatitis B is considerably less than that for hepatitis C
Which of the following statements is true regarding lifestyle modifications and prevention of spread of infection in this patient? A)The amount of alcohol that this patient consumes is insufficient to have an adverse impact on disease course B) Her sexual partner is at high risk for acquiring HBV infection, and therefore should be started on hepatitis B immune globulin (HBIG) C) The patient should receive a 2-dose series of vaccinations for hepatitis A D) The risk for sexual transmission of hepatitis B is considerably less than that for hepatitis C
Lifestyle Modifications The patient should be informed of the potential modes of transmission, including sexual transmission, blood exposure, and vertical transmission. Close contacts should be tested for HBV and should be vaccinated if not immune. Patients with HBV infection should be vaccinated for hepatitis A if not already immune. Abstinence from alcohol is advisable as there is no clear safe limit for alcohol use and they should be advised to avoid hepatotoxic medications. Risk factors for the acquisition of other viruses, including HCV and HIV, should also be addressed.
Considering this patient's clinical status and laboratory studies, • what is the most appropriate next step in management? • A) Start lamivudine 100 mg once daily • B) Start one of the "second-generation" oral antiviral medications, such as • adefovir 10 mg od, entecavir 0.5 mg od, or telbivudine 600 mg daily • C) Obtain a liver biopsy • D) Observation; readdress initiation of treatment if serum ALT increases
Considering this patient's clinical status and laboratory studies, • what is the most appropriate next step in management? • A) Start lamivudine 100 mg once daily • B) Start one of the "second-generation" oral antiviral medications, such as • adefovir 10 mg od, entecavir 0.5 mg od, or telbivudine 600 mg daily • C) Obtain a liver biopsy • D) Observation; readdress initiation of treatment if serum ALT increases
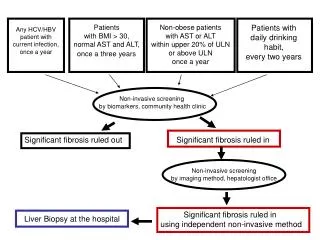
Role of Liver Biopsy Serum ALT and HBV DNA level are generally, good surrogate markers of disease activity. BUT patients may have normal serum ALT in the setting of marked inflammation and/or fibrosis on liver biopsy. HBV DNA levels generally correlate well with the degree of disease activity. However, HBV DNA levels fluctuate, and a higher viral load does not always predict advanced disease. Conversely, patients with a lower (yet still elevated) viral load may still have advanced liver disease, including cirrhosis.
.4 Baseline HBV DNA Level, copies/mL .3 Cumulative Incidence of Liver CirrhosisREVEAL HBV Study 37.1% 1.0 x 106 n=627 1.0-9.9x105 n=344 1.0-9.9x104 n=649 300-9.9x103 n=1210 <300 n=944 n=3,774 23.0% Cumulative incidence of liver cirrhosis .2 .1 10.0% 6.3% 5.2% 0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 Year of follow-up P value for log-rank test, <0.001 Uchenna H. I, et al. Gastroenterology 2006; 130:678-686
What is the most appropriate management strategy at this time? A) Start lamivudine 100 mg once daily B) Start adefovir 10 mg once daily C) Start entecavir 0.5 mg once daily D) Observation; follow liver function tests every 3 months for 1 year
What is the most appropriate management strategy at this time? A) Start lamivudine 100 mg once daily B) Start adefovir 10 mg once daily C) Start entecavir 0.5 mg once daily D) Observation; follow liver function tests every 3 months for 1 year
Which of the following statements is true regarding HCC screening in this patient? • HCC screening is not necessary because there is no fibrosis on biopsy • HCC screening should be initiated because the patient's age and sex place her at higher risk for HCC • Her ethnicity places her at higher risk for HCC than if she were of African descent • Her family history of HCC increases her risk for HCC, and therefore screening should be initiated
Which of the following statements is true regarding HCC screening in this patient? • HCC screening is not necessary because there is no fibrosis on biopsy • HCC screening should be initiated because the patient's age and sex place her at higher risk for HCC • Her ethnicity places her at higher risk for HCC than if she were of African descent • Her family history of HCC increases her risk for HCC, and therefore screening should be initiated
Case Continued Two years later the patient is seen by her GP with new complaints of fatigue and cervical lymphadenopathy. Lymph node biopsy reveals a diagnosis of non-Hodgkin's lymphoma. Chemotherapy with rituximab and CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone) is planned. Serum ALT remains within normal range and HBV DNA level at this time is < 2000 IU/mL. The patient decides to undergo chemotherapy at a hospital closer to family members who live in another part of the country. You discuss her case with the oncologist who will be assuming her care.
What are your recommendations at this time? A) Continue to follow serum aminotransferases and HBV DNA levels at monthly intervals while she is receiving chemotherapy. Begin antiviral therapy if ALT level rises to > 2 times ULN. B) Continue to follow serum aminotransferases and HBV DNA levels at monthly intervals while she is receiving chemotherapy. Start antiviral therapy if her HBV DNA level rises > 20,000 IU/mL even if serum ALT remains normal. C) Start lamivudine 100 mg once daily. Continue for at least 3 months after completion of chemotherapy. D) Given that the HBV load is undetectable, her disease is classified as inactive and she no longer needs regular follow-up at all.
What are your recommendations at this time? A) Continue to follow serum aminotransferases and HBV DNA levels at monthly intervals while she is receiving chemotherapy. Begin antiviral therapy if ALT level rises to > 2 times ULN. B) Continue to follow serum aminotransferases and HBV DNA levels at monthly intervals while she is receiving chemotherapy. Start antiviral therapy if her HBV DNA level rises > 20,000 IU/mL even if serum ALT remains normal. C) Start lamivudine 100 mg once daily. Continue for at least 3 months after completion of chemotherapy. D) Given that the HBV load is undetectable,her disease is classified as inactive and she no longer needs regular follow-up at all.
Chemotherapy and HBV HBV reactivation is common among patients receiving chemotherapy haematological malignancy > solid malignant tumors. 21% to 53% of patients who are HBsAg positive will have a flare with chemotherapy. HBsAg-positive patients are at the highest risk.
Chemotherapy and HBV BUT Patients with resolved HBV infection (ie, HBsAg-negative, HBcAb positive and HBsAb-positive) may have reactivation with immunosuppression. Worse if HBeAg-positivity High pretreatment HBV load Male sex Young age High pretreatment serum ALT The risk for hepatic decompensation is greatest during recovery from immunosuppression
Current Advice All patients undergoing chemotherapy should be screened for HBV Infection. (Flares have been seen with the use of Immunomodulatory drugs such as infliximab/rituximab) Consider Rx in hepatitis B cAb+ve patients sAg positive patients should be started on lamivudine 3 weeks before treatment Patients should have Lamivudine for 3 months after the completion of chemotherapy
Case Continued Despite your recommendation, she was not treated with preemptive antiviral therapy before initiation of chemotherapy. She was successfully treated with 6 cycles of R-CHOP (CHOP + rituximab), and her non-Hodgkin's lymphoma is thought to be in remission. Two months after completion of chemotherapy, laboratory studies revealed a rise in her serum ALT and HBV DNA levels; she was started on lamivudine 100 mg once daily for presumed HBV reactivation. Fortunately, her serum ALT normalized and HBV viral load became undetectable on lamivudine.
She has now been on lamivudine continuously for more than 1 year. Her most recent laboratory studies were as follows: AST 85 ALT 132 HBV DNA 400,000 IU/L A liver biopsy was obtained and revealed grade 2 inflammation and stage 2 fibrosis. No lymphoma was identified.
What is the most likely cause of the recent rise in this patient's serum ALT and HBV DNA load? A) Recurrent lymphoma with hepatic infiltration B) Emergence of a lamivudine-resistant strain of HBV C) Delayed hepatotoxicity from the chemotherapy regimen D) Hepatic failure from a paraneoplastic syndrome
What is the most likely cause of the recent rise in this patient's serum ALT and HBV DNA load? A) Recurrent lymphoma with hepatic infiltration B) Emergence of a lamivudine-resistant strain of HBV C) Delayed hepatotoxicity from the chemotherapy regimen D) Hepatic failure from a paraneoplastic syndrome
Extended LAM therapy in HBeAg(-) CHB:The Italian experience (616 patients) VirologicalResponse to LAM (4 Years): Resistance ExceedsEfficacy Virological response 1 Virological Breakthrough2 100 89% 80 63% 61% 60 52% 48% % patients 39% 37% 40 20 11% 0 1 year 2 years 3 years 4 years 1 HBV DNA < 105 copies/mL 2 Re-appearance of HBV DNA > 105 copies/mL Di Marco V for AISF Lamivudine Study Group, Hepatology. 2004; 40: 883-91
Which of the following is the most appropriate management strategy in this patient? • Continue lamivudine and do not add an additional antiviral agent unless serum ALT and HBV DNA level continue to increase • Continue lamivudine and add adefovir 10 mg once daily • Discontinue lamivudine and start adefovir 10 mg once daily • Begin entecavir 0.5 mg once daily
Which of the following is the most appropriate management strategy in this patient? • Continue lamivudine and do not add an additional antiviral agent unless serum ALT and HBV DNA level continue to increase • Continue lamivudine and add adefovir 10 mg once daily • Discontinue lamivudine and start adefovir 10 mg once daily • Begin entecavir 0.5 mg once daily
Rebound of serum HBV DNA >1 log10 cpm
Rise in serum transaminases Worsening of liver disease
Extended LAM therapy in HBeAg(-) GHB:The Italian experience (616 patients) Major clinical events under therapy (Hepatitic flares, decompensation,HCC, transplantation, death) Non-cirrhotics:6.5% Cirrhosis Child. A:31% Cirrhosis Child B-C:86% Di Marco V for AISF Lamivudine Study Group, Hepatology. 2004; 40: 883-91
Once Viral Resistance has developed Add or Switch?
Evolution of viral quasi-speciesduringsequentialmonotherapies WT v LAM ADV LAM LAM-R ADV-R Zoulim, Antiviral Research, 2004
ADEFOVIR Frequency ?? LAM + ADV -R Evolution of viral quasi-specieswith a de novo combinationtherapy Wild type v LAMIVUDINE LAM-R ADV-R Zoulim, Antiviral Research, 2004
What are your recommendations for following this patient? • She should remain on antiviral therapy indefinitely • Serum ALT and HBV DNA levels should be followed every 3-6 months • Screening for HCC should continue indefinitely • All of the above are appropriate recommendations for following this patient
What are your recommendations for following this patient? • She should remain on antiviral therapy indefinitely • Serum ALT and HBV DNA levels should be followed every 3-6 months • Screening for HCC should continue indefinitely • All of the above are appropriate recommendations for following this patient