classification of Periodontal Disease
500 likes | 3.31k Views
classification of Periodontal Disease. LECTURE 8 أستاذ د. رائد عزيز.

classification of Periodontal Disease
E N D
Presentation Transcript
classification of Periodontal Disease LECTURE 8 أستاذ د. رائد عزيز
The classification presented in this chapter is based on the most recent, internationally accepted, presented and discussed at the 1999 International Workshop for the Classification of the Periodontal Diseases organized by the American Academy of Periodontology (AAP). • The overall classification system is presented in (Box 1)
GINGIVAL DISEASES Dental Plaque-Induced Gingival Diseases • Gingivitis that is associated with dental plaque formation' is the most common form of gingival disease. • Gingivitis also affect the gingiva of periodontitis-affected teeth that have previously lost attachment but have received periodontal therapy to stabilize any further attachment loss.
Gingival Diseases Modified by Systemic Factors Such as the endocrine changes associated with puberty, the menstrual cycle, pregnancy, and diabetes .Hormonal changes alterations in the gingival inflammatory response to plaque. 2- Multilobulated appearance of an early pregnancy epulis(pregnancy tumor).Treatment surgical remval.
Blood dyscrasias such as leukemia may alter immune function by disturbing the normal balance of immunologically competent white blood cells supplying the periodontium. • Gingival diseases modified by malnutrition'' have received attention because of clinical descriptions of bright red, swollen, and bleeding gingiva associated with severe ascorbic acid (vitamin C) deficiency or scurvy.
Gingival Diseases Modified by Medications Gingival diseases modified by medications‘ anticonvulsant drugs induce gingival enlargement, such as phenytoin immunosuppressive drugs such as cyclosporine A, calcium channelblockers such as nifedipine, verapamil, diltiazem, and sodium valproate.
Non-Plaque-Induced Gingival Lesions Gingival Diseases of Specific Bacterial Origin Sexually transmitted diseases such as gonorrhea(Neisseriagonorrhoeae), syphilis (Treponemapallidum).
Gingival Diseases of Viral Origin • Caused by viruses, the most common herpes viruses. • Lesions appeared by reactivation of latent viruses, especially as a result of reduced immune function.
Gingival Diseases of Fungal Origin • Oral flora has been disturbed by the long-term use of broadspectrum antibiotics. • The most common oral fungal infection is candidiasis by Candida albicans,
Gingival Diseases of Genetic Origin • One of the most clinically evident conditions is Hereditary gingival fibromatosis
Gingival Manifestations of Systemic Conditions • The most important of these diseases are lichen planus, pemphigoid, pemphigus vulgaris, erythema multiforme and lupus erythematosus. As gif. of Oral lichen planus
Foreign Body Reactions Introduction of amalgam into the gingiva during the placement of a restoration or extraction of a tooth, leaving an amalgam tattoo, Introduction of abrasives during polishing procedures.
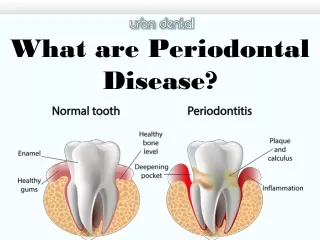
PERIODONTITIS • Three general clinical manifestations of periodontitis: • Chronic periodontitis. • Aggressive periodontitis. • Periodontitis as a manifestation of systemic diseases.
Chronic Periodontitis • Chronic periodontitis is the most common form of periodontitis • Chronic periodontitis is mostly in adults, but can be observed in children. • Chronic periodontitis is in poor O.H has a slow to moderate rate of disease progression,
Aggressive Periodontitis • Differs from the chronic form by the rapid rate of disease progression seen in • No large amount of plaque and calculus. • Healthy individual. • Family history of aggressive disease .
Clinical appearance of the periodontal tissues of a 15-year-old girl suffering from localized aggressive periodontitis. Note the proper oral hygiene conditions and the scalloped outline of the gingival margin. In the lower anterior region, the interdental papilla between teeth 31 and 32 has been lost. Intraoral radiographs (d) show the presence of localized angular bony defects, associated with clinical attachment level loss, at the mesial aspect of tooth 46, 36 and at the distal aspect of tooth 31. No significant bone loss and/or attachment loss was detectable in other areas of the dentition. Diagnosis: localized aggressive periodontitis (LAP).
Periodontitis as a Manifestation of Systemic Diseases • Hematologic and genetic disorders. • Alterations in host defense mechanisms such as neutropenia. • Leukocyte adhesion deficiencies.
Necrotizing Ulcerative Gingivitis • The defining characteristics of NUG are its bacterial etiology, its necrotic lesion. • predisposing factors such as psychologic stress, smoking, and immunosuppression. • In addition, malnutrition may be a contributing factorin developing countries.
Necrotizing Ulcerative Periodontitis • NUP: in HIV infection local ulceration and necrosis of gingiva with exposure and rapid destruction of underlying bone, spontaneous bleeding, and severe pain. HIV- patients with NUP are 20.8 times more than HIV-patients without NUP,
ABSCESSES OF THE PERIODONTIUM • periodontal abscesses: chronic or acute, gingivalor periodontal,occurring in the supportingperiodontal tissues or in the gingiva. • Periodontitis-related abscess, when the acute infection originates from a biofilm present in a deepened periodontal pocket • Non-periodontitis-related,abscess(gingival), when the acute infection from local source, such as foreign body impaction.
Endodontic-Periodontal Lesions • In endodontic-periodontal lesions, pulpal necrosis precedes periodontal changes. • A periapical lesion originating in pulpal infection and necrosis may drain to the oral cavity through the periodontal ligament, resulting in destruction of the periodontal ligament and adjacent alveolar bone. • This may present clinically as a localized, deep, periodontal pocket extending to the apex of the tooth. • Pulpal infection also may drain through accessory canals, especially in the area of the furcation, and may lead to furcal involvement through loss of clinical attachment and alveolar bone.
Periodontal-Endodontic Lesions • In periodontal-endodontic lesions, bacterial infection from a periodontal pocket root exposure may spread through accessory canalsto the pulp, resulting in pulpal necrosis. • Advanced periodontal disease, the infection may reach the pulp through the apical foramen. • Scaling and root planingremoves cementum and dentin may lead to chronic pulpitis through bacterial penetration of dentinal tubules.
THANK YOU The end