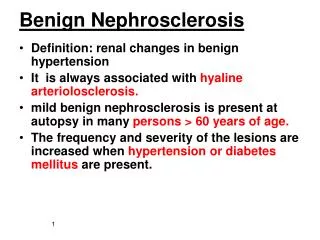
Benign liver masses
Benign liver masses. Basic workup. H&P, LFTS, AFP, CEA, CBC US, CT, or MRI Differentiate between primary hepatic malignancy vs. metastatic disease vs. benign. Hepatic abscess. Pyogenic Amebic Fungal Echinococcal. Pyogenic abscess. 80% of liver abscesses are pyogenic

Benign liver masses
E N D
Presentation Transcript
Basic workup • H&P, LFTS, AFP, CEA, CBC • US, CT, or MRI • Differentiate between primary hepatic malignancy vs. metastatic disease vs. benign
Hepatic abscess • Pyogenic • Amebic • Fungal • Echinococcal
Pyogenic abscess • 80% of liver abscesses are pyogenic • Incidence is 8-22 per 100,000 • Cholangitis is the most common cause of liver abscesses • Patient usually present with variable constitutional symptoms • US, CT, and MRI are all sensitive modalities for identifying an abscess, however they do not differentiate between pyogenic and amebic
Pyogenic abscess • Treated with antibiotics and percutaneous drainage • Open surgical drainage is reserved for patients with concurrent gastrointestinal disease processes that require surgery or those patients who have failed percutaneous drainage.
Pyogenic abscess • Almost uniformly fatal if left untreated. • Mortality rates 10-20% • Higher success rates with antibiotics and drainage vs. antibiotics and simple aspiration
Amebic abscess • Amebic liver abscess is the most common extraintestinal manifestation of the parasitic protozoan E. histolytica • The typical patient diagnosed with amebic liver abscess in the United States is a young Hispanic male between 20 and 40 years of age who has a history of travel to an endemic area or emigration from Mexico or Southeast Asia. Amebic liver abscess is much more common in men, with a male preponderance in a ratio of 10:1
Amebic abscess • Humans are the principal host, and amebiasis occurs after ingestion of E. histolytica cysts through a fecal-oral route. The main source of infection is cyst-passing chronic patients or asymptomatic carriers who transmit the cysts through water and vegetables contaminated with feces, food contaminated by fertilizers or hands of infected food handlers, or by direct transmission
Amebic abscess • The trophozoites aggregate in the liver parenchyma where, through a process of acute inflammation, granuloma formation, and progressive tissue necrosis (hence the name histolytica), an amebic liver abscess is formed. The contents of the amebic abscess, which has been classically described as “anchovy paste,” are acellular, proteinaceous debris and blood, surrounded by an outer rim of Entamoebae invading healthy hepatic tissue
Amebic abscess • Fever, hepatomegaly, and right upper quadrant tenderness are the most frequent findings on physical examination • Because most patients do not have detectable parasites in their stool, serologic testing for antibodies to E. histolytica has become the critical test for diagnosing amebic liver abscess
Amebic abscess • Ultrasound, CT, and MRI are excellent at detecting and characterizing hepatic abscesses but are incapable of differentiating an amebic abscess from a pyogenic liver abscess • A 99mTc nuclear hepatic scan is able to differentiate between a “cold” amebic liver abscess and a “hot” pyogenic abscess because of the presence of active leukocytes in the pyogenic abscess
Amebic abscess • Uncomplicated amebic liver abscess is generally treated with amebicidal drugs alone. Select patients may benefit from additional therapeutic options, including simple aspiration, percutaneous drainage, and open surgical drainage
Amebic abscess • Some experts suggest that simple aspiration should be considered in patients with (1) abscesses greater than 5 cm in size because of the increased risk of rupture, (2) abscesses located in the left hepatic lobe because of the higher frequency of peritoneal leak or rupture into the pericardium and higher mortality, (3) failure to respond to drug therapy, and (4) suspicion that the abscess may be pyogenic or secondarily infected with bacteria.
Amebic abscess • The mortality rates of patients with amebic liver abscess are reported to be from 0% to 18% • Higher mortality rates are seen in patients with delayed diagnosis, secondary bacterial infection, or complications (e.g., rupture into peritoneal, pericardial, or pleural cavity). • The overall incidence of rupture ranges from 3% to 17%
Amebic abscess • Independent risk factors associated with poorer outcomes include elevated bilirubin (serum bilirubin level >3.5 mg/dl), encephalopathy, hypoalbuminemia (serum albumin level <2 g/dl), a high volume abscess cavity (volume >500 ml), and multiple abscesses
Fungal abscess • Fungal liver abscesses are being recognized with increased frequency and currently account for approximately 10% of hepatic abscesses • Candida albicans and other Candida species are found in approximately 80% of cases • Fungal liver abscesses are usually multiple and usually occur in immunocompromised patients.
Fungal abscess • Fungal liver abscesses are treated with systemic antifungal therapy and drainage of the abscess cavity or cavities by simple aspiration, percutaneous drainage, or open surgical drainage • Amphotericin B is the first-line drug of choice for systemic antifungal therapy because of its broad fungal efficacy • Voriconazole or Caspofungin may be used to treat patients who are not responding to Amphotericin B or who have aggressive infections caused by other fungal species
Echinococcal disease • Echinococcus is a flat tapeworm • Human infestation occurs with consumption of contaminated vegetables or through contact with infected animals or soil • E. granulosus forms cysts that are constituted by an external acellular layer and an inner cellular germinal layer that produces the brood capsules containing protoscolicies, hydatid sand, or daughter cysts
Echinococcal disease • The outer acellular layer is usually 2 to 5 mm thick and is composed of fibroblasts that produce a capsule of fibrous connective tissue called the pericyst. The pericyst is calcified in approximately half of patients. • The symptoms associated with hepatic E. granulosus can vary considerably • specific enzyme-linked immunosorbent assay (ELISA) and hydatid antigen immunobinding assays yield a sensitivity and specificity up to 95% and 90%, respectively
Echinococcal disease • Chemotherapy with benzimidazole compounds (mebendazole and albendazole) is the medical treatment of choice • More recently, praziquantel, a synthetic isoquinoline-pyrazine derivative, has been used in combination with albendazole • with medical treatment alone, only 30% of patients can expect clinical and radiographic resolution. Medical treatment therefore should be used primarily in conjunction with percutaneous drainage or surgery
Echinococcal disease • For uncomplicated hydatid disease, morbidity and mortality have been reported to be in the range of 20% and 1%, • the long-term results of PAIR and surgery for hepatic hydatid cysts are excellent. Most series report recurrence rates less than 10%.
Benign Hepatic Masses • The differential diagnosis of the benign solid hepatic mass includes hepatic adenoma, focal nodular hyperplasia (FNH), focal fatty infiltration, cavernous hemangioma, and other rare neoplasms (e.g., mesenchymalhamartoma and teratoma) • Benign hepatic lesions are common, with an estimated incidence of 7% to 9%, and in one autopsy series, up to 20% of the population
Simple Cysts • Simple cysts are solitary more than 50% of the time and asymptomatic more than 90% of the time. • Size can range up to 20 cm, although most are less than 5 cm • Asymptomatic simple cysts less than 8 cm require no intervention but should be observed
Simple Cysts • Any symptoms are usually related to mass effect, causing pain in the right upper quadrant and occasionally early satiety. Rarely, intracystic hemorrhage and infection may develop • patients with symptomatic cysts (>5 cm) should undergo laparoscopic or open cyst unroofing.
Complex cysts • If multiple simple cysts are seen, consider polycystic liver disease • This is an inherited condition (autosomal dominant), often found in association with renal cysts • the majority of patients with polycystic liver disease remain asymptomatic with preserved liver function and do not require surgical intervention
Complex cysts • Biliary cystadenomas are uncommon, slow-growing complex cysts measuring up to 20 cm in size. They are benign but have malignant potential to transform into cystadenocarcinoma and thus should be surgically removed whenever recognized • The diagnosis is made by the presence of mesenchymal tissue
Complex cysts • Radiologically, internal septations are almost always seen in cystadenomas on contrast-enhanced CT or MRI. Cystadenomas have irregular borders and a thick stromal layer, and calcifications and mural nodules can occasionally be seen in the walls
Hemangioma • Autopsy series report prevalances from 0.5% to as high as 20.0%. The female-to-male ratio is between 5:1 and 6:1. Hemangioma is usually found between the ages of 30 and 70 years • tumors arise from the endothelial lining of blood vessels as vascular ectasias and have been associated with high estrogen states including puberty, pregnancy, oral contraceptive use, and androgen treatment
Hemangioma • Most tumors are less than 5 cm and asymptomatic • Contrast-enhanced CT with delayed venous examination will demonstrate peripheral nodular enhancement and progressive centripetal fill-in
Hemangioma • Hemangiomas almost never require surgical resection after the diagnosis is secure because most lesions are asymptomatic, and risk of spontaneous rupture is extremely small. • For symptomatic lesions, simple enucleation is recommended because it preserves the maximal amount of functional liver
FNH • Focal nodular hyperplasia (FNH) is the second most common benign solid hepatic tumor (behind hemangioma), comprising 8% of all primary hepatic tumors. • Prevalence of FNH is estimated to be 3% of the general population, predominantly in women in their third to fifth decades. • The female-to-male ratio is between 6:1 and 8:1
FNH • FNH consists of benign-appearing hepatocytes with cords of fibrous septae radiating from a central scar, which comprises biliary structures of hepatocellular origin • Most patients present with an asymptomatic, solitary tumor of less than 5 cm near the hepatic surface. Only 10% of patients have clinical symptoms
FNH • On contrast-enhanced multiphasic CT imaging, lesions are usually homogenous and isoattenuating to liver parenchyma before contrast injection. Lesions are bright, hypervascular with hypodense central scarring on arterial phase examination. If present, radiating hypodense fibrous bands and septa that arise from the scar are characteristic findings
FNH • Nuclear medicine imaging can sometimes be helpful to distinguish FNH from hepatic adenoma because sulfa-colloid is taken up by Kupffer cells (present in FNH), which are usually absent in adenoma
FNH • Treatment strategy is heavily influenced by the certainty of diagnosis. In asymptomatic patients with a clear diagnosis, no further treatment is necessary, and the patient may be observed. In equivocal cases in which all imaging modalities fail to establish a firm diagnosis, biopsy is warranted for histologic examination
Hepatic adenoma • Hepatic adenoma (HA) is a rare hepatic tumor that occurs predominantly in women aged 20 to 40 years, with a female-to-male ratio of at least 4:1 and reportedly as high as 11:1. • It has a strong association with oral contraceptive use, with an incidence of 3 to 4 in 100,000 oral contraceptive users versus 1 in 100,000 nonusers
Hepatic adenoma • HAs are mostly solitary (70%–80%), well circumscribed, round, and unencapsulated. A pseudocapsule is often present • Larger HA tumors (>5 cm) can be associated with right upper-quadrant pain, fullness, or discomfort. Because of its hypervascular nature and lack of a capsule, HA carries a moderate to high risk of spontaneous rupture, associated with increasing size (>5 cm). When rupture occurs, it is intratumoral in one third of cases and intraperitoneal in two thirds of cases.
Hepatic adenoma • On CT, adenomas often appear heterogeneous because of their mixed components of fat, hemorrhage, and necrosis. On portal venous examination or delayed images, they may appear isodense. HAs are contrast enhancing because of their rich vascular supply and often show peripheral enhancement with centripetal progression, indicating the presence of large subcapsular feeding vessels and early draining veins