Download
1 / 52
520 likes | 767 Views
Identifying and Intervening with Patients at High Risk of Hospital Admission Academy Health Annual Research Meeting, June 5 th 2007. Maria C. Raven, MD, MPH, MSc John C. Billings, JD Mark N. Gourevitch, MD, MPH Eric Manheimer, MD. Bellevue Hospital Center.

E N D
Identifying and Intervening with Patients at High Risk of Hospital AdmissionAcademy Health Annual Research Meeting, June 5th 2007 Maria C. Raven, MD, MPH, MSc John C. Billings, JD Mark N. Gourevitch, MD, MPH Eric Manheimer, MD Bellevue Hospital Center
High Cost Care Initiative (HCCI): Research Initiative at Bellevue Hospital Center, NYC • Supported by United Hospital Fund • Goals: • Characterize high-cost patients with frequent hospital admissions • Use data to inform intervention to reduce admissions/costs and improve care
What we’re going to cover • Why focus on high cost Medicaid patients? • How can we target high cost patients to identify them for interventions? • What we have learned from identifying patients? • What are the next steps?
High Cost Medicaid Patients: the 80-20 ruleNYC MEDICAID SSI DISABLED ADULTSMedicaid Managed Care “MMC” Mandatory [Non-Dual, Non-HIV/AIDS, Non-SPMI] 2003- 2004 Percent of Total 72.9% Patients Expenditures Source: NYU Center for Health and Public Service Research, UHF, NYSDOH, 2006.
Why Focus on High Cost Cases? • Not only is it where the money is… • These are some of the patients with the greatest need • Many moving into managed care • What used to be “revenue” is now “expense” • Improved care offers potential for cost savings
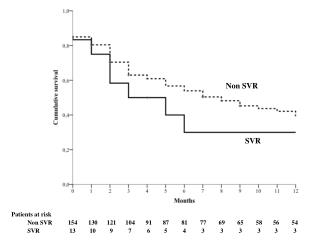
Predictive algorithm can identify high-risk patients • Predictive algorithm created by John C. Billings identifiesMedicaid patients at high-risk for hospital admission in next 12 months • Algorithm generates risk score from 0-100 for every patient in a dataset • Based on prior utilization • Higher risk scores (>50) predictive of higher risk of admission in next 12 months
General Approach for Development of Risk Prediction Algorithm (Reference) Admission Year 1 Year 2 Year 3 Year 4 Year 5
General Approach for Development of Risk Prediction Algorithm Examine utilization for prior 3+ years (Reference) Admission Year 1 Year 2 Year 3 Year 4 Year 5
General Approach for Development of Risk Prediction Algorithm Predict admission next 12 months Examine utilization for prior 3+ years (Reference) Admission Year 1 Year 2 Year 3 Year 4 Year 5
Bellevue-specific predictive algorithm • Pulled last five years of Bellevue’s Medicaid billing data • Inpatient, ED, outpatient department • Logistic regression created Bellevue-specific case-finding algorithm • Created risk scores (0-100) applicable for any patient with a visit in the past 5 years • Cohort with risk scores>50 = high risk for admission in next 12 months
Subject Enrollment • Cross-checked all admitted patients against our high-risk cohort every 24 hrs • Identified and interviewed 50 such patients and their providers during hospital admission • Determined medical/social contributors to frequent admissions • Qualitative/quantitative measures
Inclusion/Exclusion criteria • Ages 18-64 • Medicaid fee-for-service visit to Bellevue from 2001-2005 • Excluded:HIV, dual eligible, institutionalized when not hospitalized, unable to communicate
Patients enrolled when algorithm-predicted admission occurred
Interview instruments • Quantitative data from 50 patients • Demographics • SF-12 (health and well-being) • Usual Source of Care • BSI-18 (anxiety/depression/somatization) • Perceived Availability of Support Scale (social support) • Patient Activation Measure • WHO-ASSIST (substance use) • Medications (adapted from Brief Medication Questionnaire) • Qualitative data from 47 patients, 40 physicians and 16 social workers
Recruitment scheme for Bellevue pilot project Billings’ algorithm Daily computer query checked past 24 hours’ admissions against 2,618 high-risk patients
Strength of algorithm • PPV=0.67 • Of all admitted high risk patients, over 20 bounce-backs among 16 patients • Of these 16 patients, 9 eligible, 8 interviewed • 5 patients had >1 bounce-back during study period Source: NYU Center for Health and Public Service Research, UHF, NYSDOH, 2006.
Mr. O • 58 y/o man with COPD and CHF • Lives with daughter • Feels hospital admission is unavoidable when he has difficulty breathing • Does not seek intervention at symptom onset from primary doctor • Multiple admissions for COPD and CHF
Mr. R • History of over 30 detox admissions • One rehab • Homeless on street • Depression • No other medical problems
Ms. C • Severe lupus • Severe pain • Outpatient doctors won’t prescribe her the narcotics she wants/needs • Repeated admissions for lupus flare and pain control • Often with 24-48 hour stays and no changes to outpatient regimen
Housing 60%
Housing • Disproportionate admissions for substance use, mental illness, and substance use-related medical problems among homeless subjects
Substance use: ASSIST data • 74% had mid-high substance use risk scores (37/50) • Risk for harmful use/dependence with related social, legal, health problems • 14% tobacco only (7/50) • 60% multiple substances (30/50) • Majority tobacco and alcohol, followed by cocaine and opioids • 7 pts had used IV drugs
Mental Health • SF-12 Mental Composite Score • Lower scores = higher levels of anxiety and depression • Compared to the general US population: • 38% (19/50) scored below the 25%ile • 38% scored below the median • BSI-18 “cases” at high risk for psychopathology based on anxiety, depression, and somatization summary score • 68% (34/50) cases
Usual Source of care Source: High Cost Medicaid Project – Bellevue Hospital Center, NYU Center for Health and Public Service Research, 2006
Access to care Source: High Cost Medicaid Project – Bellevue Hospital Center, NYU Center for Health and Public Service Research, 2006.
How much can we pay for an intervention, and still expect to save? (or break even) • Depends on: • Risk score level • Projected reduction in inpatient admissions in the following year • Based on annual Medicaid expenditures in our cohort: • 25% reduction in future admissions over 1 year allows intervention spending of $9350 per patient
Limitations • Observational study-no control group • Limited to English and Spanish speaking, non-HIV, Medicaid fee-for service • Bellevue Hospital population • Urban, underserved
Conclusions and Implications • Patients with frequent hospital admissions comprise small percentage of all patients, but account for disproportionate share of visits and costs. • Social isolation, substance use, mental health, and housing issues were prevalent in our study population • Cited by patients/providers as contributing substantially to their hospital admissions. • Interventions focused on more effective management of their complex issues could result in cost-savings via decreased utilization and improved health.
Intervention project planning • Intervention being informed by: • Pilot data • Partnership with providers of homeless services • Successful components of similar programs in other safety net settings around country* • Meetings with community providers (CBOs) of other services (e.g. substance use, mental health, HIV) *Chicago Housing for Health Partnership, California Frequent Users of Health Services Initiative www.chcf.org
Bellevue intervention project model • Begin at patient’s bedside in hospital, continue after his/her discharge into the community • Housing component • Flexible, intensive care management model, multi-disciplinary team approach, tailored to needs of each patient • Bellevue-based team will partner with CBOs
Thank You • John C. Billings, JD • Marc N. Gourevitch, MD, MPH • Lewis R. Goldfrank, MD • Mark D. Schwartz, MD • Eric Manheimer, MD • United Hospital Fund • Supported in part by CDC T01 CD000146
Bellevue Hospital Intervention Project • Hospitalized high-risk patients identified using predictive algorithm • Small comprehensive multi-disciplinary team • Intensive assessment, arrange and follow to ensure and assist with provision of post-discharge support • Housing, residential substance abuse treatment, community based mental health treatment, specialized medical outpatient care • Provision of temporary housing while awaiting supportive housing placement/prompt placement into permanent housing
Bellevue intervention project baseline measures (RCT) • Baseline assessments: • Self-report generated Charlson Comorbidity Index: patient-reported disease severity measure predictive of 1-year mortality • Socio-demographic measures (e.g. age, gender, income, education) • Diagnoses obtained from subject’s electronic medical record
Bellevue intervention project baseline measures (RCT) • Baseline assessments (validated tools): • Health and daily functioning • Substance use • Mental Health • Support Scale • Usual Source of Care • Housing status/living situation • Common Ground in-depth assessment
Bellevue intervention outcome measures • Primary outcome • Hospital admissions and associated expenditures • Secondary outcomes • Other health services (ED, outpatient clinics) utilization • Other health services expenditures • Intervention costs • Housing status • Change in psychosocial variables • Appt adherence • Benefits enrollment • Entry into substance use services
The intervention must pay for itself • Central goal: intervention that generates more savings to the delivery system that it costs to implement and sustain. • Eliminate even small % admissions and substantial cost savings can be had. • Comprehensive economic analysis planned that considers • Changes in the numbers of inpatient admissions, ED visits, and outpatient visits during the intervention period in addition to their related expenditures • All costs related to the intervention. • Ability of intervention to succeed in this goal will help determine whether it is • Sustainable • Exportable to other sites.
Admission diagnoses: 30/50 (60%) homeless/precariously housed • 23/30 (82%) :Substance use, psychiatric, medical condition related to substance use • 9 detoxification services • 3 alcohol/drug withdrawal or intoxication • 4 psychiatric • 7 drug/alcohol-related medical diagnoses • CHF, trauma, chronic septic joint, cellulitis • 5/30: infected ulcer, chest pain, catheter infection, GI bleed, COPD • All with past or current substance use
Admission diagnoses, 22/50 (44%) housed • 1 Diabetes/coagulopathy • 3 Lupus • 5 Cancer • 1 Dialysis/pain medication related • 3 non-compliance resulting in disease exacerbation • anemia, adrenal crisis, gastroparesis • 2 Alcohol complications • Hepatitis and ESLD • 3 infections (2 PNA, 1 cellulitis) • 2 COPD/asthma • 1 ortho • 1 psych