Download
1 / 102
1.07k likes | 1.53k Views
Spinal Cord Injury, Herniated Disc & Spinal Cord Tumors. Chris Puglia, MSN, RN, CEN. Objectives. Consider the risk factors, signs & symptoms, diagnostic tests, complications, and treatments of: Spinal cord injury Herniated disc Spinal cord tumors Prioritize nursing diagnoses

E N D
Spinal Cord Injury, Herniated Disc & Spinal Cord Tumors Chris Puglia, MSN, RN, CEN
Objectives • Consider the risk factors, signs & symptoms, diagnostic tests, complications, and treatments of: • Spinal cord injury • Herniated disc • Spinal cord tumors • Prioritize nursing diagnoses • Discuss legal and ethical issues • Case study/questions
Spinal Cord Protection Bones- vertebral column 7 Cervical 12 Thoracic 5 Lumbar 5 Sacral Discs- between vertebra
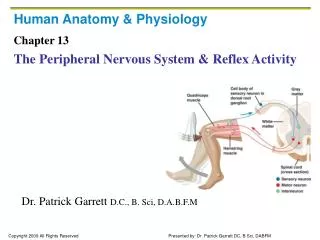
Nervous System and the Spinal Cord • ANS can be affected by Spinal Cord Injury (SCI) • Sympathetic chains on both sides of the spinal column (T1-L2) • Parasympathetic nervous system is the cranial-sacral branch (brainstem, S2-4) • Reflex Arc
Etiology of Traumatic SCI • MVC: most common cause • Other: falls, violence, sport injuries • SCI typically occurs from indirect injury from vertebral bones compressing cord • SCI frequently occur with head injuries • Cord injury may be caused by direct trauma from knives, bullets, etc
Spinal Cord Injury- SCI • Compression • Interruption of blood supply • Traction • Penetrating Trauma
Spinal Cord Injury • Primary • Initial mechanism of injury • Secondary • Ongoing progressive damage • Ischemia • Hypoxia • Microhemorrhage • Edema • Hemorrhage and edema occur in the cord post injury, causing more damage to cord • Extension of the cord injury from cord edema can occur over the first few days • watch the phrenic nerve
Spinal Shock • Decreased reflexes and loss of sensation below the level of injury • Motor loss: flaccid paralysis below level injury • Sensory loss: loss touch, pressure, temperature pain and proprioception perception below injury • Lasts days to months
Neurogenic Shock • Due to loss of vasomotor tone • SNS loss results in parasympathetic dominance with vasomotor failure • Loss of SNS innervation causes peripheral pooling and decreased cardiac output • Hypotension and Bradycardia • Orthostatic hypotension and poor temperature control (poikilothermic)
Classifications of SCI • Mechanism of Injury (MOI) • Skeletal and Neurologic Level • Completeness (degree) of Injury Mechanism of Injury 1. Flexion 2. Hyperextension 3. Compression 4. Flexion /Rotation
Classifications of SCIMechanism of Injury Flexion (hyperflexion) • Most common because of natural protection position. • Generally cause neck to be unstable because stretching of ligaments
Classifications of SCIMechanism of Injury Hyperextention • Caused by chin hitting a surface area, such as dashboard or bathtub • Usually causes central cord syndrome symptoms
Classifications of SCIMechanism of Injury Compression • Caused by force from above • Such as hit on head • Or from below as landing on butt • Usually affects the lumbar region
Classification of SCILevel of Injury Spinal cord level • When referring to spinal cord injury, it is the reflex arc level (neurologic)not the vertebral or bone level • The thoracic, lumbar & sacral reflex arcs are higher than where the spinal nerves actually leave through the opening of vertebral bone
Classifications of SCICompleteness (Degree) of Injury • Complete • Incomplete • Central cord syndrome • Anterior cord syndrome • Brown-Sequard syndrome • Posterior cord syndrome • Cauda Equina and Conus Medullaris
Classification of SCICompleteness (degree) of Injury Complete (transection) • After spinal shock: • Motor deficits • Spastic paralysis below level of injury • Sensory • Loss of all sensation perception • Autonomic deficits • Vasomotor failure and spastic bladder
Classification of SCICompleteness (degree) of Injury Incomplete Central Cord Syndrome • Injury to the center of the cord by edema and hemorrhage • Motor weakness and sensory loss in all extremities • Upper extremities affected more
Classification of SCICompleteness (degree) of Injury Incomplete Brown-Séquard Syndrome • Hemisection of cord • Ipsilateral paralysis • Ipsilateral superficial sensation, vibration and proprioception loss • Contralateral loss of pain and temperature perception
Classification of SCI Completeness (degree) of Injury Incomplete Anterior Cord Syndrome • Injury to anterior cord • Loss of voluntary motor, pain and temperature perception below injury • Retains posterior column function (sensations of touch, position, vibration, motion)
Classification of SCICompleteness (degree) of Injury Incomplete Posterior Cord Syndrome • Least frequent syndrome • Injury to the posterior (dorsal) columns • Loss of proprioception • Pain, temperature, sensation and motor function below the level of the lesion remain intact
Classification of SCICompleteness (degree) of Injury Incomplete ConusMedullaris • Injury to the sacral cord (conus) and lumbar nerve roots CaudaEquina • Injury to the lumbosacral nerve roots • Result = areflexic (flaccid) bladder and bowel, flaccid lower limbs
Clinical Manifestations of SCI • Skin: - pressure ulcers • Neuro: - pain - sensory loss - upper/lower motor deficits - autonomic dysreflexia • Cardio: - dysrhythmias - spinal shock - loss of SNS control over blood vessels - orthostatic hypotension, - poikilothermic
Clinical Manifestations of SCI • Respiratory: • decrease chest expansion, cough reflex & vital capacity • diaphragm function-phrenic nerve • GI: • stress ulcers • paralytic ileus • bowel- impaction & incontinence • GU: • upper/lower motor bladder • impotence • sexual dysfunction • Musculoskeletal: • joint contractures • bone demineralization • osteoporosis • muscle spasms • muscle atrophy • pathologic fractures • para/tetraplegia
Common Manifestation/Complications Upper and Lower Motor Deficits • Upper motor deficits result in spastic paralysis • Lower motor deficits result in flaccid paralysis and muscle atrophy
Common Manifestations/Complications • Spinal cord injuries are described by the level of the injury • the cord segment or dermatome level • such as C6; L4 spinal cord injury • Terms used to describe motor deficits • Prefix: • para- meaning two extremities • tetra- or quadra- all four extremities • Suffix: • -paresis meaning weakness • -plegia meaning paralysis Quadraparesis means what?
Common Manifestations/Complications • C1-3 = usually fatal • Loss of phrenic innervation = ventilator dependent • No B/B control • Spastic paralysis • Electric w/c with chin/mouth control
Common Manifestations/Complications • C6 = weak grasp • Has shoulder/biceps to transfer & push w/c • No bowel/bladder control • Consider level of independence
Common Manifestations/Complications • T1-6 = full use of upper extremity • Transfer self • Drive car with hand controls and do ADL’s • No bowel/bladder control
Immediate Care Emergency Care at Scene, ED & ICU • MOI • Transport with cervical collar (LOG ROLL) • Assess ABC’s • Suction PRN/Airway • O2 • BVM/Intubate • IV x2 large bore • Foley • CMS
Diagnostic Studies for SCI • X-ray of spinal column • CT with and/or without contrast (depends on MOI) • MRI • Lab work • Blood gases
Therapeutic Interventions • Medications • IV methylprednisolone (Solu-Medrol) within 8 hrs to decrease cord edema • Controversial!!
Therapeutic Interventions • Medications • To control or to prevent complications of SCI and immobility: • Vasopressors to maintain perfusion • Histamine H2 blockers to prevent stress ulcers • Anticoagulants • Stool softeners • Antispasmodics
Therapeutic Interventions Stabilization/ Immobilization Traction Gardner-wells tongs Halo Casts Splints Collars Braces
Therapeutic Interventions Surgery for SCI • Manipulation to correct dislocation or to unlock vertebrae • Decompression laminectomy • Spinal fusion • Wiring or rods to hold vertebrae together
Nursing ManagementAssessment • HEALTH HISTORY (SAMPLE) • Description of how and when injury occurred (MOI) • Other illnesses or disease processes • Ability to move, breathe, and associated injury such as a head injury, fractures
Nursing Management Assessment PHYSICAL EXAM • LOC and pupils • may have indirect SCI from head injury • Respiratory status • phrenic nerve (diaphragm) and intercostals; lung sounds • Vital signs • Motor • Sensory • Bowel and bladder function
Nursing ManagementAssessment Motor Assessment Upper Extremity • Movement, strength and symmetry • Hand grips • Flex and extend arm at elbow • with and without resistance
Nursing Management Assessment Motor Assessment Lower Extremity • Flex and extend leg at knee • with and without resistance • Planter and dorsi flexion of foot • Assess for Clonus
Nursing Management Assessment Sensory assessment • With the sharp and dull ends of a paperclip have the individual, with their eyes closed identify • Use the dermatome as reference to identify level • C6 thumb; T4 nipple; T10 naval
Nursing Problems/Interventions • 1.Impaired mobility • 2.Impaired gas exchange • 3. Impaired skin integrity • 4. Constipation • 5. Impaired urinary elimination • 6. Risk for autonomic dysreflexia • 7. Ineffective coping
1. Impaired Physical Mobility • Log roll as a single unit; provide assistance as needed to keep alignment; teach patient • Care traction, collars, splints, braces, assistive devices for ADL’s • Flaccid paralysis- use high top tennis shoes or splints to prevent contractures. Remove at least every 2 hrs for ROM (active ROM best)
1. Impaired Physical Mobility • Spastic Paralysis • Prevent spasms by avoiding: sudden movements or jarring of the bed; internal stimulus (full bladder/skin breakdown; use of footboard; staying in one position too long; fatigue) • Treat spasms by decreasing causes; hot or cold packs; passive stretching; antispasmodic medications • Assess skin breakdown & thrombophlebitis; remove TED hose at least every shift
1. Impaired Physical Mobility • Prevent/treat orthostatic hypotension • Abdominal binder, calf compressors, TED hose when individual gets up • Assess BP, especially when rising • Teach use of transfer board • Assist Physical Therapy with tilt table as individual gradually gets use to being in an upright position
2. Impaired Gas Exchange • Phrenic nerve (C3-5) controls the diaphragm bilaterally. If nerve is nonfunctioning then individual is ventilator dependent. • Thoracic nerves control the intercostals muscles for breathing and abdominal muscles aide in breathing and coughing
2. Impaired Gas Exchange • Respiratory rate, rhythm, depth, breath sounds, respiratory effort, ABG’s, O2 saturation • Signs of impending extension of SCI up cord to phrenic nerve level (C3-5) • Need for ventilatory assistance (tracheotomy, ventilator ) • Quad cough (assistive cough) as needed
3. Impaired Skin Integrity • Change position frequently • Protection from extremes in temperature • Inspect skin at least 2x/day especially over boney prominences • Avoid shearing and friction to soft tissue with transfers • Removal of TED hose every 8 hours/SCDs • Nutritional status
4. Constipation • Bowels rely more on bulk than on nerves • Stimulate bowels at the same time each day. Best after a meal when normal peristalsis occurs • Individual may progress from Dulcolax suppository to glycerin then to gloved finger for digital stimulation • Assess bowel sounds prior to giving food for the first time– paralytic ileus!