Download
1 / 55
550 likes | 779 Views
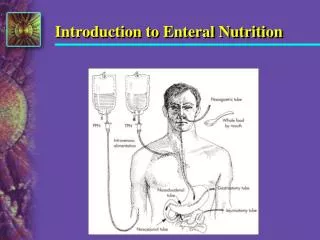
Enteral Nutrition might save life. Where Should We Feed critically ill patients?. Done by Dr KHALED AL SEWIFY MD, MRCP, EDIC. Artificial Nutritional Support. Enteral nutrirition. Preserves the intestinal mucosal integrity : Maintains mucosal immunity.

E N D
Enteral Nutrition might save life Where Should We Feed critically ill patients? Done by Dr KHALED AL SEWIFY MD, MRCP, EDIC
Enteralnutrirition • Preserves the intestinal mucosal integrity : • Maintains mucosal immunity. • Prevents of increased mucosal permeability. • Decreases bacterial translocation. Marik, Zaloga CCM 2005
Theory of BT • SB and colon contain 1010 anaerobes and 107 Gram +ve and Gram -veaerobes and Enough Endotoxins to kill us 1000 X. Magnotti & Deitch 2005 JOABA
Saving lives in severe sepsis with the help of enteral nutrition EN enriched with eicosapentaeonicacid, ɣ-linolenic acid & antioxidantsin ARDS patients with severe sepsis mortality with ARR of 19.4%. Pontes-Arruda-Crit Care Med,Sept.2006; 34. 2325-2333. Pontes-Arruda-Crit Care Med 2006; 34. 2325-2333.
Ventilator Free days////ICU Free days P < 0.001 7.6 more ventilator-free days 6.2 more ICU-free days
Advantages of gastric feeding • It is more physiological, is easier to begin and more convenient. • Spare both gastropancreatic reflexes and gastrin release. • Buffers gastric acid well.
What are The Problems Associated with Gastric Feeding in Critical Illiness ?
Incidence of UGIT Intolerance to Gastric Feeding Mentec H (2001)– Crit Care Med 29 : 1955-1961
What are the sequelae of upper GIT intolerance to enteral nutrition?
Prospective survey in Australian ICUs De Beaux (2001)EN in the critically ill : Anaesth. Intensive Care 29:619-622
Hazards of UGIT Intolerance Incidence of Nosocomial Pneumonia • 2-Patients with Upper GIT Intolerance Had Increased Incidence Of Nosocomoial Pneumonia Feeding intolerance
Hazards of UGIT Intolerance Mortality Rate • 2-Patients With Upper GIT Intolerance Had Increased • Mortality Feeding intolerance
Hazards of UGIT Intolerance ICU Length Of Stay • 4-Patients With Upper GIT Intolerance Had Longer Duration of ICU Stay Feeding intolerance
So probably the gastric feeding may not always be as safe as it is sometimes considered. • The net result is Aspiration Syndrome. Heyland DK 199-AM J RespirCrit Care Med 159:1249-1256.
Aspiration Syndrome 1. 70% with altered LOC. 2. > 70% of trauma patients at injury. 3. > 40% of patients with EN. Bowman, et al CCNQ 2005
Prokinetic therapy for feed intolerance in critical illnes : one drug or two ? • Erythromyicin is superior to Metoclopramide. • Combination therapy had greater feeding success, received more daily calories, and had a lower requirement for postpyloric feeding & less incidence of tachyphylaxis. • Should be considered as first line therapy in treatment of feed intolerance in criticall illness. * Reignier J -Crit Care Med.2002, 30:1237-1241. *Nguyen NQ - Crit Care Med. 2007 Nov;35(11):2561-7.
What is new ? • Motilin derivatives : # Long term efficacy is unknown. # Very rapid tachyphylaxis. • Cholecystokinin antagonist :Loxiglumide # Very recent. # Accelerate gastric emptying in healthy humans. # No trials in critically ill patients. * Castllo E, et al .Am J Physiol 2004;287:G363-G369 * CremoniniF,etal.Am J Gastroenterol 2005;100:625-663
? ? ? ? • Where Best To Deliver Enteral Nutrition In Critically Ill Patients ? • Is Small Bowel Feed The Answer ? • What Are The Advantages Of Small Bowel Feed?
Advantages of Small Bowel Feed • Improved absorptive capacity. • Less impairment of motility. • Better respiratory function as it prevents gastric distension. • Greater distance between the delivery site and the pharynx & respiratory tree.
Conclusions OF THE META-ANALYSIS • Small bowel feeding compared with gastric feeding: *Associated with a reduction in pneumonia . *Improves calorie and protein intake and is associated with less time taken to reach target rate of EN. *No difference in mortality or MV days. Drover JW - Gastrointest Endosc Clin N Am - 01-OCT-2007; 17(4) : 765-75
Comparison of early gastric and post-pyloric feed in ccritically ill patients : a meta-analysis • By contrast to the previous meta-analysis there was no significant benefits on the risk of diarrhea, length of ICU stay, mortality or risk of aspiration pneumonia. Intensive Care Med 2006 ; 32:639
Canadian Clinical Practice Guidelines Recommendations Routine use of SB feedings in units where SB access is feasible. In units where obtaining access involves more logistic difficulties, SB feedings should be considered for patients at high risk for UGIT intolerance. When obtaining SB access is not feasible, SB feedings should be considered for selected patients with high gastric residuals repeatedly and are not tolerating gastric feed. Heyland DK - JPEN J ParenterEnteralNutr 2003;27:355- Updated Jan 2007
Benefits in head injury • Grahm et al also found a decrease in infectious complicationsfor patients with head injuries who received early enteral feedinginto the jejunum. Grahm T, Zadrozny D, Harrington T. The benefits of early jejunalhyperalimentation in the head-injured patient. Neurosurgery. 1989;25:729–735
Benefits in acute pancreatitis • By bypassing the mouth, stomach and duodenum, jejunal feeding minimize the stimulation of pancreatic exocrine secretions . • Accumulating evidence has suggested that post-pyloric feeding is safe and may also reduce complications. *Ragins, H . Am J Surg 1973; 126:606. *Wolfe, BM. Surg Gynecol Obstet 1975 Feb;140(2):241-5.
Blind placement of SB tube • Erythromycin appeared useful in 3 studies but metocopramide only in one trial. • A recent systemic review concluded that erythromycin should be administered when blindly placing a small bowel tube. *Booth CM. A systemic review of the evidence.Critc Care Med 2002,30:1429-1435. *Griffith DP . A double blind, RCT . Crit Care Med 2003,31:39- 44.
Non blind Placement of SB tube • Flouroscopy ensures 90% post pyloric and more than 50% into the jejunum. • Endoscopically-placed tubes appear to have the highest success rates 98% for tube placement into the jejunum. • US guided, 67% duodenal. • EMG guided. *Davis AR . Critic Care Med 2002, 30: 586- 590 * G Gubler, et al.Endoscopy 2006.Dec.;38 (12):1256-60
EMG Guided Post Pyloric Tube Chest. 2004;125:587-591.)
TIGER TUBE • Provides high insertion success rates (>90%). • Cost effective. • Self migrating. • So it will be left in the stomach and it will migrate peristalsis to the jejunum. Samis AJ,. Evaluation of 3 different strategies for post pyloric placement of enteral feeding tubes. Intensive Care Med 2004, 30:S 149( abst)
Bengmark Tube • Very effective : #92.5% crossed the pylorus #89.14% reached the first jejunal loop #3.4% in the duodenum #7.5% stopped in the stomach • Reached final position within 5.2 hours, 8% instantly and all within 24 hours. • Start feed immediately G Mangiant, et al.Chir Ital. ;52 (5):573-8