Lecture 4 CATARACT & GLAUCOMA
660 likes | 731 Views
Lecture 4 CATARACT & GLAUCOMA. Lecture is delivered by Ph. D., associate professor Tabalyuk T.A. Classification of cataracts: By age: congenital, juvenile, age-related (senile)

Lecture 4 CATARACT & GLAUCOMA
E N D
Presentation Transcript
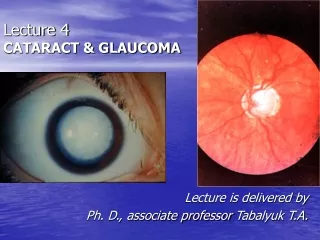
Lecture 4 CATARACT & GLAUCOMA Lecture is delivered by Ph. D., associate professorTabalyuk T.A.
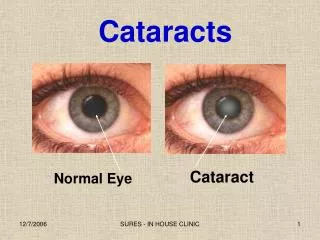
Classification of cataracts: By age: congenital, juvenile, age-related (senile) By location opacities in the lens as seen with slit beam: cortical, nuclear, anterior subcapsular, posterior subcapsular By maturity: early, immature, mature, hypermature (Morgagnian cataract) By pattern: cuneiform (typical senile type), zonular, polar, pyramidal (congenital types)
DIFFERENTIAL DIAGNOSIS The same sign is progressive (not acute) painless visual loss
Artiphakia is a condition of eye with artificial lens (IOL). Aphakia is a condition of eye without lens. The visual acuity without correction is very poor – 0,02-0,04. Iridodenesis (iris vibration) is typical. Thick plus glasses are needed for vision: for far distance – sph convex 10,0-12,0 D for near distance – sph convex 13,0-15,0 D. Secondary cataract occurs eventually in about 20 % cases after cataract surgery. It is opacity of natural posterior capsule. It can be treated by YAG laser capsulotomy. Attention! The term «complicated cataract»is used to describe a lens opacity which occurs as a result of some other disease of the eye. Longstanding uveitits, an untreated retinal detachment or an intraocular tumour are all examples of an associated disease.
CONGENITAL CATARACTS : I degree – visual acuity is 0,3 and more; the size of opacity is less then 1,5 mm; the surgery may be done at the age of 14-16 years. II degree– visual acuity is 0,05-0,2; the surgery is usually done at the age of 3-4 years. III degree– visual acuity is less then 0,05; the surgery must be done during first year of life.
Ectopia lentis (displacement of the lens) may be partial (subluxation) or complete (luxation). Aethiology: trauma, familial ectopia lentis (may be associated with ectopic pupil), associated with other ocular disprders (aniridia and buphtalmos), Marfan’s and Weill-Marchesani syndromes, metabolic (homocystinuria and hyperlysinaemia). Clinical features: iridodenesis (vibration of iris) and not proportional depth of anterior chamber. Marfan’s syndrome: tall person with partial displacement of the lens (subluxation), fragile bones and arachnodactyly.
The outflow pathways of aqueous humor: • Main: posterior chamber - pupil - anterior chamber - trabecular meshwork - Schlemm’s canal (scleral sinus)- vorticose veins – scleral venous plexus. • Additional: • 2. Perivascular spaces of iris. • 3. Suprachoroidal space - perivascular spaces – through sclera into the tenon’ s space. • 4. Perivascular spaces of central retinal vessels. • The IOP is maintained by a balance between aqueous inflow and outflow &usually measures between • 16-26 mm Hg (using tonometr of Maklakov) & • 10-20mm Hg (using tonometr of Goldman)
Not every increasing of IOP is glaucoma. It may be ocular hypertension, caused, for example, by using corticosteroids, intoxication or climax. Typical for ocular hypertension are: • absence of structural and functional changes; • lasting existence without complaints; • symmetrical increasing of IOP. • So, ocular hypertension is a symptom, glaucoma is a syndrome. • Glaucoma is such increasing of IOP, which is accompanied by specific visual defects (constriction of nasal visual field, Bjerrum’s scotoma) and specific optic disc changes (dislocation of vessels, increased cuppingetc.)
Congenital glaucoma (or hydrophtalmos) is caused byabnormal development of eye drainage system. The accumulation of aqueous in the eye due to elasticity of baby’s external coat causes the increasing of eye size. • There are 2 clinical forms: • Hydrophtalmos without stasis (megalocornea, stretching out of limbus, deep anterior chamber, increased eye, loss of vision, increased IOP, typical changes of optic nerve). • II. Hydrophtalmos with stasis (all above mentioned signs + photophobia, blepharospasmus, mixt injection, corneal oedema, which is reliefed by 40 % glucosae). • There are 4 stages: • I. Early – D of cornea 12,0-12,5 mm, anterior-posterior distance of the eye is increased on 1,5-2,0 mm, N fundus. • II. Advanced - D of cornea 13,0-14,0 mm, anterior-posterior distance of the eye is increased on 3,0-4,0, glaucomatous cupping of optic disc ophthalmoscopically. • III. Far advanced - D of cornea is more then 14,0 mm, anterior-posterior distance of the eye is more then 30,0 mm, atrophy of optic disc ophthalmoscopically. • IV. Terminal (or buftalm) – full blidness, scleral staphyloma.
Methods of diagnostic of congenital glaucoma: • General examination, especially of cornea & limbus • Biomicroscopy or focal lighting • Keratometry • Tonometry • Ultrasound biometry • Ophthalmoscopy • Methods of treatment of congenital glaucoma: • Only surgical. Immediatly! • Goniotomy • Sinusotrabeculectomy • Enucleation in buftalmos
Stages of primary glaucoma (according to visual functions defects): I – visual field is consticted less then 10 degrees, physiological cupping is increased. II - visual field is consticted more then 10 degrees, edge excavation. III – tube visual field (15 degrees from the point of fixation), edge excavation. IV – visual field or visual acuity is zero, atrophy of optic disc. Depending on IOP (using tonometr of Maklakov) glaucoma is subdivided: A (compensated) – IOP is less then 27 mm Hg. B (subcompancated) – IOP is 28-32 mm Hg. C (decompancated) – IOP is 33 mm Hg and more. According to dynamics of visual functions during 6 month: stabile & nonstabile – constriction of visual field on 10 degree and more; in tube vision – on 2-3 degrees and more; increasing of scotomas size; increasing of size of optic disc cupping
Open-angle glaucoma • Pathogenesis – constriction or closing of openings in trabeculae & Schlemm’s canal as a result of endocrine, vascular or general diseases such as atherosclerosis, artery hypertension, diabetus mellitus etc. • Clinical features:usually asymptomatic until significant loss of visual field has occured; • the eye looks usual, only dystrophic iris changes may be revealed biomicroscopically; • open anterior chamber angle on gonioscopy, may be excess pigmentation of trabeculae; • & typical for glaucoma signs (elevated IOP+visual field loss,first of its nasal part +optic nerve damage). • Methods of investigation: • Functional – visometry, perimetry, campimetry, adaptometry. • B. Objective – general examination, focal lighting, biomicroscopy, gonioscopy, ophthalmoscopy, tonometry.

![[Glaucoma] Classification](https://cdn1.slideserve.com/2649686/glaucoma-classification-dt.jpg)