Gradual visual loss
Gradual visual loss. Three common causes outside of diabetes and hypertensive retinopathies Age-related Macular Degeneration (AMD) Cataract Glaucoma. Gradual visual loss Glaucoma (primary open angle).

Gradual visual loss
E N D
Presentation Transcript
Gradual visual loss • Three common causes outside of diabetes and hypertensive retinopathies • Age-related Macular Degeneration (AMD) • Cataract • Glaucoma
Gradual visual lossGlaucoma (primary open angle) • 2% of the population >age of 40 will have either raised intra ocular pressure or glaucoma (higher in areas with a high ethnic minority population). • This rate increases to 10% of the population over the age of 75. • 33% of all referrals for glaucoma from optometrists were found to have a positive glaucoma diagnosis • ‘Estimates based on official population projections and epidemiological prevalence surveys, predict that the number of glaucoma cases in England and Wales will increase by a third by 2021, and then continue at a similar pace to 2031’
Gradual visual lossGlaucoma (primary open angle) • Reduced efficiency of trabecular meshwork • Diagnosis – 2 out of 3: • Field loss ( needs specialist assessment) • >0.7 or unequal C/D ratio • Increased IOP > 20 mmhg
Glaucoma treatment • Medical (topical) • beta-blockade ‘…ol’ (↓ production aq.) • prostaglandin‘…prost’(↑ trabecular blood flow) • Sympathomimetics ‘..ine’(↓production & ↑trabecular outflow) • Carbonic anyhdrase inh. ‘…ide’ (↓production ) • Miotics ‘piolcarpine’ (↑trabecular outflow by opening up meshwork) • Medical (systemic) • Carbonic anyhdrase inhibitors
Glaucoma treatment • Surgical • Trabeculectomy : incision in superior portion of the scleral – iris junction to create a bleb (trap-door), underlying trabecular meshwork removed free aq humour drainage to bleb.(Mitomycin or 5FU injected to delay healing, scarring and failure) • 80% of cases no further treatment • 15% of cases, drops still needed • 5% of cases, a further operation
Gradual visual lossCataracts • cataract are gradual increasing blurred and cloudy vision, and glare – nuclear or cortical. • day case Surgery is a highly successful but more limited value if the patient also has another eye condition • By the age of 75, a quarter of all people will have developed a cataract and ‘Action on Cataracts – Good Practice Guidance’ (DH 2000) estimates that annually 3.2% of those aged 65 and over would benefit from cataract surgery
CATARACT • Red reflex ? • +7 dioptres • Visual acuity? • Pin Hole?
Gradual visual loss • Age related Macular Degeneration (AMD) • most common cause of irremediable serious loss of central vision in people over 65 years of age • more predominant in females, smokers and people with long term exposure to sunlight • Prevalence of 15% by the age of 75 with increase of approximately 35% over the next 20 years
Gradual visual loss-AMD • dry (atrophic) and wet (exudative) • no treatment for dry AMD but it is usually less severe and more slowly progressive than the wet form which can be rapid and result in irreversible scarring of parts of the retina. • Wet / exudative -formation of new sub-retinal vascular complexes, Leakage causes rapid loss of vision within 2 years
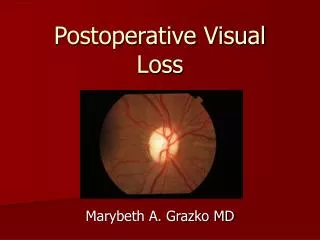
Gradual visual lossAMD • Treatment • Dry -no treatment is of proven, but progress may be slow and may stabilise. However,may enter the exudative stage at any time. Amsler chart Some interest in dietry supplements (ADREDS) – high dose Zinc and anti-oxidants (plenty of green veg and stop smoking!) • Magnification, illumination, low visual aids
Wet - laser photocoagulation of subretinal neovascular membrane. Borders of the identified by fluorescein angiography. Recurrence is common -12-15% per year • subfoveal difficult to rx – near fixation (Photodynamic therapy comprising verteporfin plus laser activation = new approach being evaluated • Ranibizumab - a recombinant, humanized, monoclonal antibody ‘fab’ that neutralizes all active forms of vascular endothelial growth factor A- has been evaluated for the treatment of neovascular age-related macular degeneration
AMD Amsler Normal AMD
Middle ear disease • Middle ear disease • ET normal function and causes of dysfunction • Development of CSOM • Age and prevalence • Sequele of CSOM • Examination • Management • PCT guidelines
E/T Dysfunction Resolution Negative middle ear pressure Acute perforation Acute serous otitis media Acute otitis media Chronic serous otitis media Atelectatic drum segment in pars tensa Attic retraction pocket Chronic Perforation Cholesteatoma Aural Polyp
Sequele of CSOM Chronic perforation Retraction Pocket
E/T dysfunction resolution Resolution
Middle Ear Disease • PCT guidance on grommets (BEN) • Refer if deafness/ recurrent infections >3/12 • Operation if no resolution in 3-6/12 or drum changes or deafness • Return as soon as possible to watchful waiting : in Primary or Secondary care