Download

1 / 19
190 likes | 381 Views

E N D
SPINAL INJURIESFractures and dislocations of the spine are serious injuries as they may be associated with damage to the spinal cord. Commonest site of spinal injuries is the thoraco-lumbar segment; followed by the cervical spine.20% of spinal injuries result in neurological deficit – quadriplegia in the cervical region and paraplegia in the throcalumbar spine. These injuries lead to prolonged morbidity or death.Functional anatomy of spine.Basically segmented cylindrical structure which serves three main functions.Protection of spinal cordSupport of TrunkTransmission of weight of head, upper limbs and trunk to the pelvis and lower limbs.
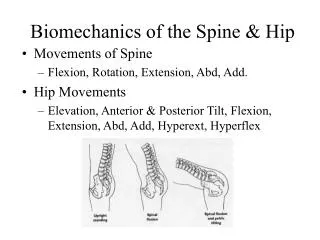
Movements in the spine: • Forward flexion • Extension • Lateral flexion • Rotation Stability of the spine: • The 3 column concept • Anterior column • Middle column • Posterior column
Anterior: • Anterior longitudinal ligament • Anterior part of annulus fibrosus • Anterior half of vertebral body Middle: • Posterior half of the annulus • Posterior half of vertebral body and • Posterior longitudinal ligament Posterior: • Posterior bonny arches and • Spinus ligaments • When only one column is disrupted e.g. wedge compression of a vertebral the spine is stable. When two or three columns are disrupted the spine is unstable.
Classification of spinal injuries • Flexion injuries – commonest e.g. wedge compression • Flexion rotation injuries – subluxation and dislocation • Vertical compression – Burst fracture • Extension – commonly vertical compression • Direct e.g. stab wound • Indirect due to violent muscle contraction • Flexion distraction seat belt injury Causes of spinal injuries • R.T.A 36% • Domestic and industrial accidents 37% • Falls – Stair case • Ladders • Trees • Sports injuries 20.5% - Diving into shallow water • Self harm and criminal assault 6.5%
Association injuries • Head injuries with coma lasting 6hr. 7% • Chest injury – Requiring active treatment 20% • Abdominal injuries 2.5% requiring laparotomy • Multiple injuries 24% Clinical features • History of trauma • Pain/Tenderness at the neck or back radiating because of nerve root irritation • Bruising at the back/neck • Palpation gap (step) along the spinal column • Sensory disturbances distal to neurological level • Weakness/flaccid paralysis below this level
In cervical spine injuries • Spinal concussion = spinal shock Lasts 24hrs – 8-10 days • sensory loss below the level • flaccid paralysis • visceral paralysis • loss of reflexes • loss of anal reflex • If relaxes do not return after 24 hrs = complete spinal cord injury. Cord injuries – classification • complete spinal cord injuries • - Spinal shock • Incomplete • anterior cord syndrome • anterior part of spinal cord usually injured by flexion rotation force or compression fracture of the vertebral body. It is often associated with anterior spinal artery compression.
Central cord syndrome – Hyperextension injury • usually elderly people • classifiably flaccid weakness arms and spastic in the legs • Sacral sensation and bowel function often spared • Posterior cord syndrome – Hyperextension with fracture posterior column Good power pain and temperature sensation. • Brown sequard syndrome – Stab injuries • - Hemisection of the cord. • Power is decreased or absent on the side of the injury pain and temperature normal. contralateral – normal power with in prick and temperature decreased or absent.
MANAGEMENT I • Spinal cord injury is a mortal condition and has been recognized as such since antiquity. The annual incidence of spinal cord injury in U.K. is 10-15 per million of the population. • Although the effect of the initial trauma is irreversible the spinal cord is at risk from further injury by injudicious early management. • Pain relief is provided by opioids titrated slowly iv. The patient should be moved by 4 people at a time • Neurological examination must include: • Sensation to pin prick • Sensation to fine touch and joint position sense • Power of muscle group MRC scale (medical research Council Scale) • Reflexes (abdominal, anal, bulbocavenus as well • Cranial nerves • The level and completeness of neurological damage are assessed.
Other examination • Rectal sensation • Rectal motor – sphincter contracts over gloved finger • Bulbocavenus relaxes • Squeeze glass penis • Anal sphincter contracts A.B.C of Resuscitation • Use of antibiotics not used routinely unless in established infection • Bladder or • Skin • Steroids as early as possible within 8 hrs methyl paednisolone 30mg/kg iv then followed hourly at 5.4 mg/kg 1hr for 23 hrs • Pain relief – Opioids titrated iv • Also nonsteroidal anti-inflammatory drugs • antispastics • stabilize e.g. cervical traction 8 weeks then wean unto – Minerva Jacket or stiff cervical collar
Skeletal – Gardner wells or • - Cruthfield tongs • Skin traction equivalent – Halter traction Investigation • i. X-ray – AP, Lat, Oblique lat. • Open mouth views • ii. Myelogram – Incomplete lesion • iii. C.T. Scan • iv. M.R.I. • v. Laboratory investigation. X-ray fracture patterns • Wedge compression • Burst fractures • Chance fracture compare transverse fracture in long bones • Translational
MANAGEMENT II • Aims • To Realign the spine • Prevent further damage (unstable injury) • Aid neurological recovery • Obtain and maintain spinal stability • Aim at early functional recovery Treatment of complications of spinal cord injuries • Spacticity • Paralised bladder • Bed sores • Bowel programme • Psychological problem • Family and relations • Joint contracture • Loss of job • Thrombo embolism • Spacticity and paraarticular hetrotopic calcification:- Management is by drug and excision of calcification.
Paralised bladder:- they have two problem one is automatic and autonomous bladder. Acute retention will develop in quadriplegia unless the sacral segment are spared. • Bed sores Management:- As a result Ischaemia cause by pressure on the skin. Treatment includes daily dressing and skin grafting. • Bowel programme:- Aim at reflex emptying of bowel with suppositories • Psychological and sexual function problem:- Treatment includes Psychotherapy and family education. • Physiothgerapy:- Joint contracture and stiffness. Treatment includes, move joint passively over the arrange of movement • Loss of job:- Occupational therapy
Thrombo embolism:- Drug treatment • Thoracolumbar injuries • Thoracolumbar body jacket if the skin is sensate use pillow arrangement to nurse the patient in spinal bed. • Bladder – Intermittent Cathreisation followed by indwelling cathre changed every 2 weekly. • avoid infection • calculi formation Later – Automatic bladder • UMNL Residual urine is small • The emptying is involuntary • Level of injury is above S2 Autonomous bladder • LMNL • Level at or below S2 • Reflex centre loss intrusive bladder reflexes take over • Emptying voluntary • Large volume of urine