Immunological Diseases
Immunological Diseases. Spectrums and Mechanisms Assistant Professor Kiat Ruxrungtham, M.D. Division of Allergy and Clinical Immunology Department of Medicine, Faculty of Medicine Chulalongkorn University. Principles of Immunology. Key roles of immune responses Terminology


Immunological Diseases
E N D
Presentation Transcript
Immunological Diseases Spectrums and Mechanisms Assistant Professor Kiat Ruxrungtham, M.D. Division of Allergy and Clinical Immunology Department of Medicine, Faculty of Medicine Chulalongkorn University
Principles of Immunology • Key roles of immune responses • Terminology • Primary and Secondary Immune Responses • Cells and Molecules involved • Immunological Disorders • Mechanisms and Clinical Implications
Key Roles of Immune System • Prevent and control infection • Prevent and control autoimmune diseases • Prevent and control malignancy • Prevent and control allergic diseases • Prevent and control graft-versus-host (GVH)
Terminology • Antigen, allergen, immunogen and epitope • Innate and Acquired Immunity • Allergy • Autoimmunity, autoimmune diseases
Innate and Acquired Immunity Innate Acquired Ag specificity no yes Magnitude (10, 20) same higher (20 > 10) Memory no yes Key components PMN, NK T, B lymphocytes C’, barriers APCs
Primary IR 7-10 relatively low Mostly IgM relatively high Secondary IR 2-5 days relatively high Other class (IgG, IgA, etc) relatively low Primary and Secondary Immune Responses Lag period Peak response Ig class Antigen [ ]
Cells and Molecules Involved in Immunology Innate Immunity • Cells: epithelium, phagocytes (neutrophils, monocyte-macrophages) NK cells, mast cells • Molecules: complement, inflammatory mediators, cytokines, chemokines, adhesion molecules
Cells and Molecules Involved in Immunology Acquired Immunity • Cells: APCs (macrophages), T (CD4+, CD8+) and B lymphoctyes (plasma cells), monocytes • Molecules: HLA, cytokines, immunoglobulins, adhesion molecules
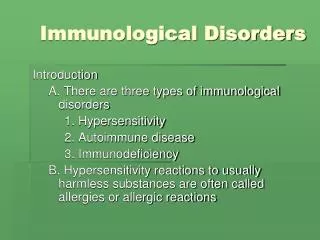
Immunological disorders • Hypersensitivity mediated disorders • Immunodeficiency : 10 and 20 ID
Classification of Hypersensitivity Gell and Coomb’s Classification: 4 Types • Type 1 : IgE-mediated • Type 2 : Cytotoxic antibodies • Type 3 : Ag-Ab Immune complexes • Type 4 : Delayed-type, cell-mediated hypersensitivity
Type I Hypersensitivity • Allergen exposure, sensitization and re-exposure • IgE antibody, mast cells/ basophils and its’ mediators • Target organ immediate reactions • Clinical allergy: atopic diseases, drug allergy, insect allergy and anaphylaxis
Pathogenesis of Allergic Disease Genetic Susceptibility • Adjuvant factors: • Tobacco smoke • Air pollutants • Lack of protective • factors: • Infection ? • Immunization ? • Nutrition ? Allergic Sensitzation Allergen Exposure Upper/lower airway or Skin hyperresponsiveness Pollutants Infection Excercise Vary in spectrum and severity Allergic Diseases Modified from Ulrich Wahn 1998
Principle Pathogenesis of Allergic Diseases Durham and Till 1998, Lu 1998, Drazen 1996 APC Allergen CD4+ T-cell IL-12 Allergen Th-1 Th-2 IL-4 IgE IFN-g IL-5 IL-3 GM-CSF B-cell B-cell CD8+ cell IgG Mast cell IL-5 Other cells _ + Eosonophil MBP ECP, LTs Late Phase Reaction Tryptase, LTs AllergyChula
Pathogenesis of Allergic Diseases Cells & Molecules Involved in Allergic Inflammation Modified from Robert Davies
Histamine Tryptase Chymotryptase Heparin/Chondroitin Kininogenase Chemotactic Factors Prostaglandins Leukotrienes PAF Histamine RFs IL-3, 4, 5, 6, 7, 8 GM-CSF, TNFa Chemokines -MCP1, MIP1 Oxygen radicals Mediators of Mast Cells and Basophils Secondary Mediators Primary Mediators AllergyChula Sim TC, Grant JA 1996
Mediators of Mast Cells and Allergy Urticaria, Angioedema Laryngeal edema, Shock Blood Vessels H, PGD2, LTs, PAF Kinin Bronchospasm Abd. pain, Vomiting Smooth Muscles H, PGD2, LTs, PAF Diarrhea, Rhinorhea Bronchial secretion Mucus Glands H Mast Cell Basophil Sensory Nerves Itching LTB4 PAF IL3, IL5 Chemokines Leukocytes Inflammation - LPAR AllergyChula
โรคภูมิแพ้ที่พบบ่อย โรคภูมิแพ้ทางจมูก Allergic Rhinitis โรคหืดจากภูมิแพ้ Allergic Asthma โรคภูมิแพ้ทางผิวหนัง Atopic Dermatitis โรคลมพิษUrticaria โรคแพ้อาหาร Food Allergy การแพ้ยา Drug Allergy Allergy Chula 1999
Epidemiology of Allergic Diseasesin Thai Children พยนต์ บุญญฤทธิพงษ์ และมนตรี ตู้จินดา 2533; ปกิต วิชยานนท์ และคณะ 2541
สิ่งแวดล้อม กับ โรคภูมิแพ้ ฝุ่นบ้าน ฝุ่นบี่นอน สัตว์เลี้ยง เชื้อรา เกสร ที่กักฝุ่น อาหาร ตัวไร่ฝุ่น สิ่งเหล่านี้มีอยู่รอบตัวเรา มีทั้งในบ้านและนอกบ้าน แต่มีหลายอย่างที่เราหลีกเลี่ยงได้ หากเรารู้วิธีที่ถูกต้อง
ควันบุหรี่ ควันธูป
Factors Affecting Clinical Outcomesof Allergic Diseases • Treatment • Anti-inflammatory • Anti-allergic • Relievers • Enivronmental • Allergens • Irritants • Westernization Genetic Degree of atopy • Compliance • Avoidance • Medication uses • Infection • Viral • Bacterial Allergen Immunotherapy Allergic Diseases Future Therapy ? Remission Mild Severe Moderate AllergyChula
Clinical Uses of H1 Antagonists Generation of Antihistamines Clinical First Second and Third Allergic Rhinitis ++ ++ (better compliance) Urticaria ++ ++ (better compliance) Atopic dermatitis ++/+++ ++ (better compliance) Asthma - -/++(Meta-analysis= NS)URI/NAR ++ - Itching dermatosis ++/+++ ++ Anti-motion sickness ++ - Antiemetic ++ - Appetite stimulation ++ -(+ for astemizole) Insomnia ++ - AllergyChula
Treatment of Allergic Rhinitis in Adults Allergy 1994; suppl. 19
Treatment of Allergic Asthma Allergy 1994; suppl. 19
Type II Hypersensitivity • Cytotoxic antibodies: IgG, IgM • Mechanisms of cytolysis: Fix complement and/or ADCC • Clinical spectrums: • Autoimmune Hemolytic anemia (AIHA) • ABO Miss-matched • ITP • Stimulatory antibody: Grave’s disease • Inhibitory antibody: Myasthenia gravis (anti-Ach Rc)
Principle treatments in Type II • ABO matching • For AIHA, ITP: Steroid, immunosuppressive agents, +/- splenectomy
Type III Hypersensitivity • Mechanisms: Ag (protein, drugs) + Ab (IgG, IgM) --> Immune complex --> deposit at subendothelial basement membrane --> fix complement --> chemotaxis ---> PMNs --> vasculitis • Immune complex diseases: • Serum sickness • Autoimmune diseases: prototype-SLE • Vasculitis
Principle treatments in Type III • Serum sickness: Avoidance of heterogeneous protein injection: ERIG antirabies • Autoimmune diseases: SLE • Avoidance sun exposure • Steroid • Immunosupressive agents
Type IV Hypersensitivity • Delayed-type cell-mediated reaction • Mechanism: Antigen (contactants) --> sensitized T-lymphoctyes --> re-exposure --> T cells activation --> cytokines ---> mononuclear cell recruitment --> DTH • Clinical disorder: Atopic contact dermatitis
Principle treatments in Type IV • Avoidance • Topical steroid • Systemic steroid, if severe