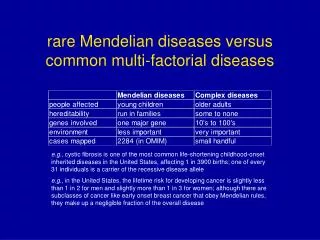
Download
1 / 55
560 likes | 675 Views
Anesthesia for Rare Co-existing Diseases. Alexandru Apostol, M.D. Achondroplasia. The most common cause of Dwarfism Autosomal dominant Mutations of FGFR3 receptor Large head, facial hypoplasia, spine deformation, trident hand. Achondroplasia & Anesthesia.

E N D
Anesthesia for Rare Co-existing Diseases Alexandru Apostol, M.D.
Achondroplasia The most common cause of Dwarfism Autosomal dominant Mutations of FGFR3 receptor Large head, facial hypoplasia, spine deformation, trident hand
Achondroplasia & Anesthesia Difficult IV, mask ventilation, intubation Risk for Cervical cord ischemia OSA, CSA, PHTN Restrictive lung disease GERD Difficult RA
Angelman SyndromeHappy Poppet Syndrome Mutation of UB3A gene, abnormal GABAR Developmental delay Movement dysfunction Minimal speech, nonverbal communication Microcephaly, seizures Prognathia
Angelman & Anesthesia Dysregulation of GABA, NMDA, AMPA Difficult RA Bradycardia Syncope Seizure disorder
Apert SyndromeAcrocephalosyndactyly Malformation of the skull, hands, feet and face Mutation of fibroblast growth factor receptor 2 gene Craniosynostosis, Brachycephaly, mid -face hypoplasia, Hypertelorism, increased ICP,syndactyly Cardiac defects, polycystic kidney, pyloric stenosis OSA, CSA
Apert Syndrome & Anesthesia Difficult IV Difficult mask ventilation High incidence of Bronchospasm No reported difficult intubations Might need CPAP post op Avoid sedatives and Opiods
Arthrogryposis Multiplex Congenita Intrauterine fetus joint contractures, 3 degrees of severity Type 1 affects extremities Type 2 affects extremities + scoliosis+ CDH Type 3 affects CNS
Arthrogryposis Multiplex Congenita & anesthesia Difficult IV Spinal and caudal might be difficult Possible cervical spine instability 25% difficult intubation Difficult positioning for surgery Risk of bleeding if on Valproic acid
Central core diseaseShy-McGee Syndrome Inherited dominant neuromuscular disorder= congenital myopathy 25% association with MH Hypotonia, motor developmental delay, with predominantly proximal weakness Cardiomyopathy rare When associated with scoliosis echo and PFTs are needed
Central core disease & Anesthesia MH avoidance technique (no Succinylcholine no volatile anesthetics) TIVA and RA are safe Neurological consult before RA for Juridical reasons Pre-op CK level may be helpful Higher intr-aop blood loss during scoliosis surgery
CHARGE SyndromeHall – Hittner Syndrome Coloboma Heart defect Atresia Choanae Retarded Growth and Development Genital Hypoplasia Ear Anomalies/Deafness Cleft lip and palate TEF
CHARGE Syndrome & Anesthesia Inhalation induction may be difficult RSI preferred Difficult intubation Risk of aspiration Risk of arrhythmias Prolonged post-op mechanical ventilation
Duchenne muscular dystrophyDystrophinopathy Most common & severe muscular dystrophy Mutation in dystrophin gene on Chromosome Xp21 Progressive skeletal muscle weakness Fatty and fibrous infiltration of muscles Age of diagnosis 3-5 years Risk of aspitation Cardiomyopathy (TEE)
Duchenne muscular dystrophy & Anesthesia GA with TIVA Prolonged muscle relaxant effects Avoid Succinylcholine and VA Risk of hyperkalemic cardiac arrest or sever rhabdomyolysis No risk of MH short use of VA is possible Avoid NO2 in case of cardiac involvement RA can be done
Epidermolysis bullosa Group of inherited diseases with trauma induced blister formation of skin and mucosa Deficiency of structural proteins of the dermo -epidermal junction Microstomia, ankyloglosson and dental decay Cardiomyopathy GERD Anemia
Epidermolysisbullosa & Anesthesia Difficult airway Prevent friction and trauma, lubrication of FM, LMA, ETT, secure ETT with non adhesive LMA, ETT one seize smaller Extensive padding Infection prophylaxis Good pre-op sedation, RSI RA is OK but less skin infiltration with LA Patting the skin for disinfection
Kasabach-Merritt SyndromeHemangioma-Thrombopenia Vascular lesion with consumptive coagulopathy and throbocytopenia Vascular tumor with irregular nodules Pt on Steroids, Vincrstine, Interferon, Ticlopidine and or Aspirin Avoid Platelet transfusion due to trapping in the tumor Heart failure secondary to massive AV shunts
Kasabach-Merritt & Anesthesia Difficult airway No nasal intubation Avoid platelet transfusion Correct coagulopathy ( fibrinogen, tranexamic acid) Side effects from Chemotherapy RA (aware of thrombocytopenia)
Mucolipidosis II and III Lysosomal storage disease Defective N –acetylglucosamine 1-phosphotransferase Accumulation of carbohydrate, lipids in various tissues and organs The phenotype resemble Hurler Syndrome Jaw and neck may be stiff Short neck Thickened epiglottis, enlarged adenoids Cardiomyopathy, PHTN
Mucolipidosis II and III & Anesthesia Difficult airway , FOI Difficult LMA ETT smaller than predicted Difficult IV OSA
Prader-Willi SyndromePrader-Labhardt-Willi Syndrome Genetic disorder of chromosome 15 Hypothalamic-Pituitary abnormality Hypotonia in infancy, hyperphagia, morbid obesity Behavioral problems OSA Cardiomyopathy Seizure disorder
Prader-WilliSyndrome & Anesthesia Difficult airway management Difficult landmarks for RA Difficult IV High risk for bronchospasm High risk for aspirtation Potential for prolonged effects of NMB Safe to use succinylcholine Ketamine can be use with caution
Russel - Silver SyndromeRussel - Silver Dwarfism Genetic etiology of chromosome 7 and 11p15 Growth retardation Face and limb asymmetry Relative macrocephaly prominent for-head Hypospadias Anterior and small larynx Subglottic stenosis Retrognathia and hypognathia Risk of hypoglycemia
Russel - Silver Syndrome & Anesthesia Difficult airway due to facial dysmorphysm, retrognathia, hypognathia, small mouth opening, Difficult mask ventilation RA can be used Ambulatory surgery is not recommended
WelanderDistal Myopathydistal myopathy Swedish type Autosomal dominant Almost exclusively found in Sweden and Finland Late adult onset Weakness and atrophy of distal muscles Inability to extend the fingers Decreased DTR No cardiac involvement
Welander Distal Myopathy & Anesthesia GA and RA not contraindicated PT with RLS no Etomidate or Propofol Careful use of NMB
Prolonged Q-T Interval SyndromeJervell and Lange-Nielsen SyndromeRomano-Ward Syndrome It can be congenital or acquired Causes of acquired are :Quinidine, Disopyramide, TCA, SAH, hypokalemia, hypomagnesaemia, right neck dissection The pathognomonic feature is prolonged Q-T more than 0.44 sec on EKG even when corrected for HR Can present as Syncope, or sudden death due to VT Asymmetric sympathetic innervation of the right and left heart
Prolonged Q-T and Anesthesia BB can shorten QT interval Left stellate ganglion block can transiently shorten Q-T for acute cardiac arrhythmias Surgical Ganglionectomy is successful if the block work EKG pre-op for children with congenital deafness or Hx of sudden death in the family GA might trigger ventricular Dysrhythmias if not on BB pre-op Electrical defibrillator should be available Phenytoin can shorten Q-T can be given po after surgery
AT A GLANCE... • Mimics of MH • Diseases Associated with MH • Possibly MH-Related • Rhabdomyolysis but not MH • Muscle Biopsy & IVCT • MHAUS, NAMHR, NMSIS • & MH Hotline • Bibliography Epidemiology of MH Pathogenesis of MH 4 Different Case Scenarios The MH Clinical Grading Scale MH-like Anesthetic Events
“Epidemiologic barriers” in defining the true incidence of MH” Difficulty in establishing diagnosis of MH No noninvasive diagnostic screening test
“Epidemiologic barriers” in defining the true incidence of MH” (cont.) All cases are not reported to MH Registry Triggering of MH in susceptible patients may not occur Lack of uniform criteria for MH diagnosis
Incidence of Different Forms of MH in Relation to Type of Anesthesia Fulminant MH Abortive MH Overall incidence (all subgroups of suspected MH included) Total number of anesthetics 1:251,063 1:17,435 1:16,303 General anesthesia 1:221,811 1:15,404 1:14,403 Anesthesia with potent inhalation agent 1:84,488 1:6,653 1:6,167 With succinylcholine 1:61,961 1:4,506 1:4,201 Without succinylcholine 1:174,597 1:20,541 1:18,379 Anesthesia with administration of succinylcholine 1:140,006 1:8,819 1:8,297
Pathogenesis: Key Concepts Heterogeneous disorder Genetically transmitted with variable expression/penetrance Can be triggered by volatile anesthetics and succinylcholine
Hereditary - multiple genes Several chromosomes: • 19q11.2-13.2 Ryanodine (RyR1) • Release of Ca2+stores from sarcoplasmic reticulum • 17q11.2-q24 • Altered sodium channel functioning • 7q21.1 • Dihydropyridine (DHP), voltage sensor for RyR1 • 1q32 • CACNL1A3 gene encoding the alpha 1-subunit of the voltage-gated DHP receptor that interacts with RyR1
Non-specific clinical presentation Hypercarbia Tachycardia Fever Hyperventilation Metabolic and Respiratory Acidoses Cardiovascular collapse Rhabdomyolysis
Case One in PACU A 13 year old boy underwent 2 hours of uncomplicated General Anesthesia.
Case Two in OR A 10 year-old male was given Propofol & Rocurronium to facilitate tracheal intubation. Anesthesia was continued with Isoflurane/N2O.
Case Three Masseter Rigidity? A 16 year-old male who refused spinal anesthesia for lower extremity surgery, was given Propofol and Succinylcholine (no Volatile Anesthetic gas).
Case Four Outside Tobin JR, Jason DR, Nelson TE, Sambuughin. Malignant Hyperthermia and Apparent Heat Stroke N. JAMA 2001; 286(2):168-169 http://jama.ama-assn.org/issues/v286n2/ffull/jlt0711-4.html A 12 year old male collapsed after rigorous exercise.
Process Indicator Points 1. Rigidity Generalized muscular rigidity 15 Masseter spasm________________________________ 15 2. Muscle Breakdown Creatine Kinase >20,000 IU after succinylcholine 15 Creatine Kinase >10,000 IU with no succinylcholine 15 Cola colored urine in perioperative period 10 Myoglobin in urine > 60 mcg/L 5 Myoglobin in serum > 170 mcg/L 5 Blood/plasma/serum K> 6 mEq/L no renal ills _____ 3 3. Respiratory Acidosis PETCO2 > 55 mmHg with controlled ventilation 15 ArterialPaCO2 > 60 mmHg, controlled ventilation 15 PETCO2 > 60 mmHg with spontaneous ventilation 15 ArterialPaCO2 > 65 mmHg, spontaneous ventilation 15 Inappropriate hypercarbia, Anesthesiologist’s call 15 Inappropriate tachypnea__________________________ 10 4. Temperature Increase Inappropriately rapid increase 15 Inappropriately increased temperature > 38.8C_______ 10 5. Cardiac Involvement Inappropriate sinus tachycardia 3 Ventricular tachycardia or fibrillation_________________ 3 6. Family History Positive family history in first degree relative 15 Positive family history, more distant relative ____ 5 7. Others Arterial base excess more negative than –8 mEq/L 10 Arterial pH <7.25 10 Rapid reversal of MH signs after iv dantrolene 5 Positive MH family history with another indicator from the patient’s anesthetic experienceother than increased CK 10 Elevated CK and a family history of MH______________ 10 Click for larger picture Larach MG, Et Al, MH Clinical Grading Scale,Anesthesiology 1994; 80:771-9
20-34 Somewhat greater than likely 35-49 Very likely >50 Almost certine CGS Sum and Probability of MH
Case 1 Case 2 Case 3 Case 4 Rigidity 0 0 15 15 Muscle Injury 15 15 15 0 Respiratory 0 15 0 15 Temperature 10 0 0 15 Cardiac 3 0 0 15 Family History 0 0 0 0 Other 10 5 0 0 SUM 38 35 30 45 Clinical Grading Scores (CGS)
MYOPATHY INCIDENCE AGE at Dx Duchenne 0.0020 5 (<16) yrs Becker 0.00036 12 (4-19) Myotonia Dystrophica 0.000135 < 14 years MH-Like Anesthetic Events
MH Thyrotoxicosis Pheochromocytoma ETCO2 +++ ++ ++ HR +++ +++ +++ BP + ++ +++ Rigidity ++ +/- - Acidosis +++ - + Differential Diagnosis
Some Mimics of MH Adverse drug reactions Arthrogryposis Carnitine palmitoyl transferase deficiency CNS diseases Contrast media in CSF Elevated ETCO2 with laparoscopic cases Cystinosis Glycogen storage disease Lymphoma Mitochondrial disease Neuroleptic malignant syndrome Viral myopathy William’s syndrome
Diseases Associated with MHS Central core disease Isolated elevation of creatine kinase King Denborough syndrome
Possibly MH Related • Dystrophinopathy • Emery Dreifuss MD • Fascio-Scapulo-Humeral MD • Abnormal Muscle Enzymes • Ion Channel Mutations • Na, K, Cl
Rhabdomyolysis, but NOT MH • Brody’s disease • Deficient calcium adenosine triphosphatase • Mc-Ardle’s disease • Myophosphorylase B deficiency