Download
1 / 28
280 likes | 564 Views
Testicular Cancers. Ashray Gunjur Intern, Royal Melbourne Hospital. Did you know?. That the words testify, testimonial and testament are derived from. Anatomy. http://www.aboutcancer.com/testicle_anatomy1.jpg. Differentials. HISTORY? * Pain?? * Time course of symptoms?

E N D
Testicular Cancers AshrayGunjur Intern, Royal Melbourne Hospital
Did you know? • That the words testify, testimonial and testament are derived from...
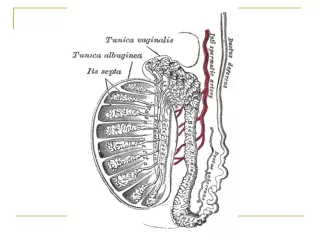
Anatomy http://www.aboutcancer.com/testicle_anatomy1.jpg
Differentials HISTORY?* Pain??* Time course of symptoms? PHYSICAL EXAM?* pain?* reducibility?* Lie of teste?
Differentials Toronto Notes 2010
Differentials • 1) Hydrocele
Differentials • 2) Epidydymal cyst/Spermatocele
Differential • 3) Varicocele
Typical case • Young man with painless growth of unilateral teste • On examniation, firm nontender, non-transilluminating mass in one of the testes
Epidemiology • Relatively rare- 1-2% of men, but.. • Most common malignancy in age 20-40 • Three peak model: infancy, 30-34 years, >60 years
Risk factors • Cryptorchidism- 4-8x risk of germ cell tumour • Risk still increased after orchiopexy in pt <6yrs old- 2.23x* • Risk still increased in contralateral testis- 5-20% of malignancy in normal descended testis! • Prior testicular cancer- 500x • Approx 1-2% of testicular cancer patients will develop a second primary contralaterally... *PetterssonA, Richiardi L, Nordenskjold A, Kaijser M, Akre O. Age at surgery for undescendedtestis and risk of testicular cancer. N Engl J Med. May 3 2007;356(18):1835-41
Risk factors • Genetics • E.g. Klinefeltersyndrom (47XXY)- germ cell tumours • Diethylstilbestrol (DES) exposure in utero • E.g. ‘Agent Orange’, Industrial occupation
Diagnosis • Best first testhypoechoic lesion
Diagnosis • Gold standard? - inguinal orchidectomy!!
Histologic types Germ cell tumors (>95%): Seminoma (40%) versus Non seminomatous germ cell tumors (NSGCT) (40%) vs. mixed (15%) Non-germ cell tumors (rare, <5%) Leydig cell tumors (precocious puberty) Sertoli cell tumors Mixed sex chord-stromal tumors
Germ cell tumours • Seminoma (40%) • Generally favourable prognosis, tend to be in older men • Rarely make B-HCG (15%), no aFP (0%) • Non-seminoma (40%) • Choriocarcinoma (elevated b-HCG (50%), haematogenous spread) • Embryonal cell • Teratoma (mature and immature) • Yolk sac (elevated AFP)
Tumour markers • AFP levels are elevated 50%-70% NSGCT • hCG levels are elevated in 40%-60% NSGCT. • AFP has a half-life of 5-7 days • hCG has a half-life of 36 hours. • Important to follow response after orchiectomy • LDH is non-specific measure of tumor burden
Risk stratification • Good-risk nonseminoma • Testicular or retroperitoneal primary tumor, and • No nonpulmonary visceral metastases, and • Good markers; all of:Alpha-fetoprotein (AFP) < 1,000 ng/mL, and • Human chorionic gonadotropin (hCG) < 5,000 IU/mL (1,000 ng/mL), and • Lactate dehydrogenase (LDH) < 1.5 times the upper limit of normal • Intermediate-risk nonseminoma • Testicular or retroperitoneal primary tumor, and • No nonpulmonary visceral metastases, and • Intermediate markers; any of:AFP 1,000 to 10,000 ng/mL, or • hCG 5,000 IU/L to 50,000 IU/L, or • LDH 1.5 to 10 times the upper limit of normal • Poor-risk nonseminoma • Mediastinal primary, or • Nonpulmonary visceral metastases, or • Poor markers; any of:AFP > 10,000 ng/mL, or • hCG > 50,000 IU/mL (10,000 ng/mL), or • LDH > 10 times the upper limit of normal
Risk stratification • Good-risk seminoma • Any primary site, and • No nonpulmonary visceral metastases, and • Normal AFP, any hCG, any LDH • Intermediate-risk seminoma • Any primary site, and • Nonpulmonary visceral metastases, and • Normal AFP, any hCG, any LDH • Poor-risk seminoma • No such thing!!
Treatment Post Orchidectomy… Seminoma Stage IA and B: radiation therapy vs surveillance (? Chemo) NSGCT Stage IA retroperitoneal lymph node dissection vs surveillance Stage IB retroperitoneal lymph node dissection vs surveillance vs chemotherapy Higher stages-chemo, f/b surgery as needed
Why? • Non-seminomas are more aggressive than seminomas • RPLND is used to guide chemotherapy • No of +ive nodes correlates to cycles of chemo
Surveillance NCCN guidelines • CT q 2-3 months for first year or two • Then q4, q6 • Labs, CXR q month for year one, then q 2 months, etc • Issues are compliance, anxiety
Question 1 The most common presenting complaint for a testicular cancer is:a) a painless swelling of a single teste b) a red, painful scrotumc) haematuriad) back pain
Question 2 • All of the following are a risk factor for testicular cancers, save • Cryptorchidism • Maternal DES exposure • Caucasian race • Repeated testicular trauma
Question 3 The following statements are false, save • Testicular cancer is the most common cancer of infancy • There are more men aged 15-25 diagnosed with testicular cancer than >50 • Unilateral surgical orchidectomy precludes the chance of testicular cancer recurring • Unilateral surgical orchidectomy is the gold standard diagnostic procedure for testicular cancer
Question 4 Routine workup and staging of diagnosed testicular cancer should include: • a-FP • B-HcG • CT A/P + C • PET scan
Question 5 The following are incorrect about Seminomas, save • Ultrasound features often involve heterogenous cystic components • aFP is often raised and used for prognostication • Para-aortic radiotherapy is often indicated • Patients with metastatic disease have a poor prognosiss