Download

1 / 1
10 likes | 125 Views
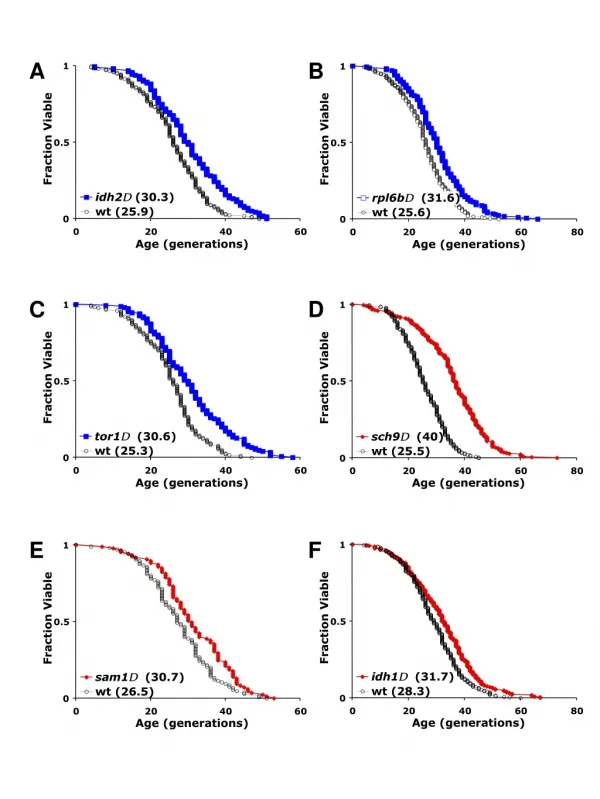
This study investigates a case of secondary membranous nephropathy (MN) triggered by an immune response to recombinant arylsulfatase B (rhASB) in a patient with mucopolysaccharidosis type VI. Following enzyme replacement therapy (ERT), the patient experienced nephrotic syndrome resistant to steroids. A combined immunosuppressive regimen including corticosteroids, rituximab, and methotrexate was used to induce tolerance to rhASB. This approach allowed ERT to resume without increasing antibody levels or worsening proteinuria, highlighting the need for tolerance induction in similar cases.

E N D
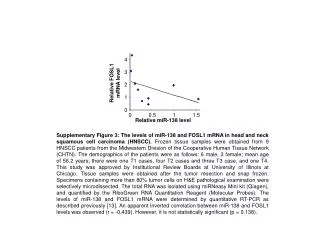
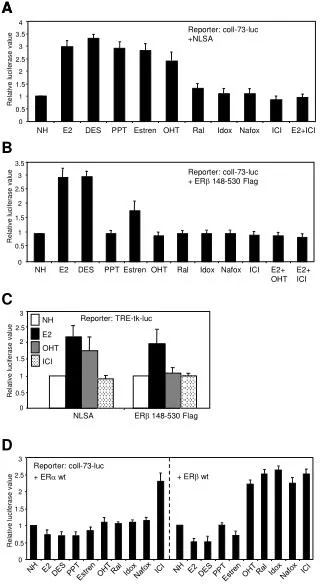
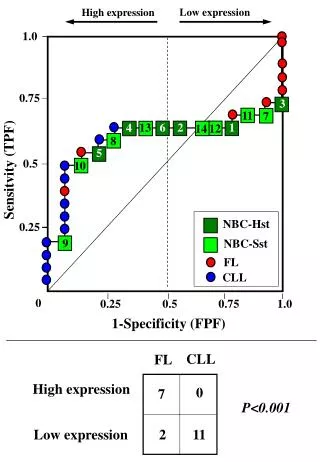
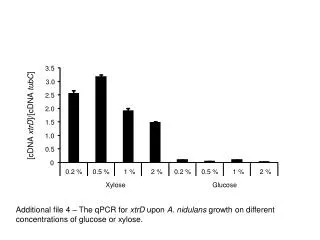
60 mg/m²qd 4 weeks + 3 MP pulses Progressivelytapered to 2.5 mg qod DEC 2010 Steroids Allo-Immune Membranous Nephropathy and Recombinant Arylsulfatase Replacement Therapy: A Need for Tolerance Induction Therapy MAR 2010 Rituximab 1 2 3 4 5 6 1 2 3 4 72 SEP 2010 IV Ig 55 AVR 2010 Methotrexate rhASB dose 1mg/kg 1mg/kg 0.5 mg/kg/week Hanna Debiec, Vassili Valayannopoulos, Olivia Boyer, Laure-Hélène Nöel, Patrice Callard, Hélène Sarda,Pascale de Lonlay, Patrick Niaudet, Pierre Ronco IgG3 • INSERM UMR_S 702, F-75020, Paris, France Reference Center for Inherited Metabolic Diseases, • Necker-Enfants-Malades Hospital, AP-HP, F-75015, Paris Descartes University, Paris, France SUMMARY This work identifies a new antigen responsible for secondary membranous nephropathy (MN) in a patient with mucopolysaccharidosis type VI due to aryl sulfatase B (ASB) deficiency. Enzyme replacement therapy (ERT) started at the age of 4 years (dose 1mg/kg/week) dramatically improved clinical manifestations. Sixteen months later and one week after orthopedic surgery, the patient who had a high anti-rhASB antibody titer, suddenly developed nephrotic syndrome resistant to steroid therapy. The kidney biopsy revealed glomerular deposition of IgG, mostly IgG4, C3 and C5b-9 in a granular pattern typical of MN. Double immunofluorescence staining with anti-rhASB and anti-human IgG showed that subepithelial granular deposits contained rhASB co-localized with IgG. Ig eluted from the patient’s biopsy specimen reacted specifically with rhASB. ERT was discontinued, proteinuria progressively decreased, but the patient's clinical condition markedly deteriorated. Induction of tolerance to rhASB was initiated by co-administration of low-dose corticosteroids, rituximab, intravenous immunoglobulins and oral methotrexate. ERT was resumed after nine months, eight weeks after starting immunosuppressive therapy, without inducing a rebound of antibody titer or an increase in proteinuria. We conclude that the allo-immune response to the recombinant enzyme is the cause of the disease. Considering the critical requirement for ERT in patients with such enzyme deficiencies, immune tolerance induction should be advocated in the patients with allo-immune MN. Patient Antenatal manifestations of storage disorder (hygroma coli, pericardial effusion) confirmed at birth: dysmorphic features, hepatomegaly Diagnosis of aryl sulfatase B (ASB) deficiency = mucopolysaccharidosis type VI (MPS VI) or Maroteaux-Lamy syndrome Enzyme replacement therapy (ERT) was started at age 4 IV rhASB (Naglazyme®, Biomarin) : 1mg/kg/week. Results (1st year) better general condition reduced frequency of ENT infections liver volume normalized growth improve infusion well tolerated and no infusion related reactions were noted reduction in urinary GAG ( biomarker) Light microscopy and immunofluorescence study of specimens of the first kidney biopsy (August 2008). He developedmembranousnephropathy Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y At age 4 1/2 years : orthopedic surgery and post-surgical immobilization (June 10, 2008) A week following surgery (June 17, 2008): nephrotic syndrome No reportedrenal complications in MPS VI or in patients receivingrh ASB • Y A B Glomerular basement membranes have diffuse spikes and clubber aspects (Jone’s staining) Electron microscopy showing subepithelial electron dense deposits C E D C5b-9 IgG C3 Glomerulus with diffuse, finely granular deposition of IgG, C3 and C5b-9 along the outer surface of all capillary walls. Patient has anti-rhASB antibodies in serum, and rhASB and anti-rhASB in glomerular immune deposits. A B C 0.3 mg/kg kDa 1 2 3 4 Time course of administration of rhASB and combined therapy Equal amounts of rhASB were resolved by SDS-PAGE and incubated with patient’s serum (1), normal serum (2), and sera from patients with membranous nephropathy (3) and IgA nephropathy 4 (A). Surgery 10-JUN-08 NS 17-JUN-08 Other patients on rhASBenzymotherapy had low titer of anti-rhASB antibodies or were negative (B). Distribution of rhASB-specific IgG subclasses in the patient’s serum (C). IgG4 IgG1 IgG2 Anti-rhASBIgG antibody titer measured by ELISA. Staining of the second kidney biopsy (March 2009) with anti-IgG subclass antibodies E F H G E Anti-rhASB antibody revealed granular staining along capillary loops only in our patient (A). Shows an adjacent section in which the anti-rhASB antiserum was preincubated with 20µg of rhASB protein (B). Patient with idiopathic MN (G). C B A Proteinuria (g/g creatinine) Urinary GAG (mg/mmolcreatinine) 0.3 mg/kg 0.5 mg/kg/week Time course of proteinuria and urinary glucosaminoglycan ( GAG) excretion J K I NS 17-JUN-08 A B C 1 2 kDa 72 Whydidthis patient develop MN? 55 • IgG was eluted from the patient’s second kidney biopsy (1) and from a patient with MN (2). Only IgG eluted from the patient’s biopsy identified rhASB. Shortlyafter surgery Beforesurgery Confocal images of cryosections of the patient’s second kidney biopsy specimen which have been double-labeled with rabbit polyclonal anti-rhASB antibody (A green) and anti-human IgG antibodies (B red). (C) Shows the merged image. Naglazymeistaken by podocytes Naglazymeismainlytrapped in GBM Other patients Effect of anasthetics Immune complexresorptionexceeds formation Y Increasedpermeability to IgG Y Y Y Integrity of the glomerular filtration barrier and function of podocytesisdestroyed Immune complex formation exceedsresorption The research leading to these results has received funding from the European Community’s Seventh Framework Programme (FP7/2007-2013) under grant agreement n° 2012-305608 (EURenOmics)