Download
1 / 13
130 likes | 308 Views
U 74 - 1807. #EGH 74-4670 No clinical information. 68 YOM. Was sent from Norwood for evaluation of Acute Renal Failure and worsening extremities edema. His Baseline Cr was 300’s (Aug06). the day of admission his Cr was 650’s

E N D
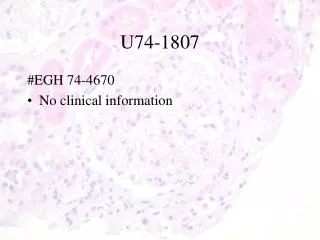
U74-1807 #EGH 74-4670 • No clinical information
68 YOM • Was sent from Norwood for evaluation of Acute Renal Failure and worsening extremities edema. • His Baseline Cr was 300’s (Aug06). the day of admission his Cr was 650’s • Was sent to UofA hospital for evaluation of Acute on Chronic Renal Failure.
PMH: • SLE: Not Biopsy proven, ds-DNA neg • MPGN: Biopsy done in 1974 • CAD: S/P CABG few years ago (5 vessels) • Cirrhosis: based on U/S. not biopsy. etiology NASH vs. Cryptogenic Cirrhosis • Seizure • Gout • HTN • Dyslipidemia • 3rd Degree Heart Block DDDR pacemaker • A.Fib ex- warfarin therapy (Warfarin was D/C on Aug)
Labs: (day of admission) • 97 41 INR: 1.4 5.8 AG 16 4.6 22 630 ALT&AST:45 & 46 T. Bili: 20 UNa 63 93 Urine S/G: 1.013 8.8 252 .28
Hospital Course: • With Diagnosis of Acute on Chronic (pre-renal) patient was started on Lasix 40 Q day and Spironolactone 100 mg QD then Lasix 80 BID. • U/O: 1000 cc/day (average) • R IJ was placed and HD started.
Light microscopy (slides are not available) 2 glomeruli showing: • Moderately severe membrano-proliferative changes: • Mesangial cell hyperplasia in axial regions of tufts • Swelling of podocytes and endothelial cells • Patchy thickening of glomerular basement membranes • Capillary lumina are narrowed • Hypertrophy and hyperplasia of parietal epithelial cells • Peri-glomerular fibrosis
IF • IgG- Moderate to marked granular deposits. • IgA- Trace amounts. • IgM- Trace amounts. • C- Moderate to marked granular deposits.
Original diagnosis (1974)Renal Biopsy: • Membrano-proliferative glomerulonephritis, • Process is active • Most consistent with a diagnosis of immune-complex induced GN
Upon review of EM pictures • EM supports a diagnosis of post-infectious or membranous GN. • Presence of numerous subepithelial deposits, somewhat more irregularly spaced than would be usual for membranous.