Template for QIPP Ideas
Template for QIPP Ideas. Headline / Title: . Streamlining the HR Recruitment process . Short description: Streamlining the Recruitment process and improving the quality of the appointments should improve productivity and increase the quality of patient care. QIPP elements*. Making it happen.

Template for QIPP Ideas
E N D
Presentation Transcript
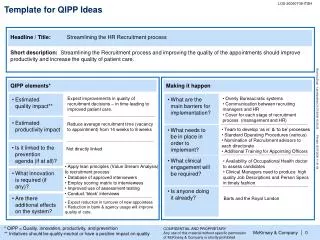
Template for QIPP Ideas Headline / Title: Streamlining the HR Recruitment process Short description: Streamlining the Recruitment process and improving the quality of the appointments should improve productivity and increase the quality of patient care. QIPP elements* Making it happen Expect improvements in quality of recruitment decisions – in time leading to improved patient care. • Overly Bureaucratic systems • Communication between recruiting managers and HR • Cover for each stage of recruitment process (management and HR) • Estimated quality impact** • What are the main barriers for implementation? • Estimated productivity impact Reduce average recruitment time (vacancy to appointment) from 14 weeks to 8 weeks • Team to develop ‘as is’ & ‘to be’ processes • Standard Operating Procedures (various) • Nomination of Recruitment advisors to each directorate • Additional Training for Appointing Officers • What needs to be in place in order to implement? • Is it linked to the prevention agenda (if at all)? Not directly linked • What clinical engagement will be required? • Availability of Occupational Health doctor to assess candidates • Clinical Managers need to produce high quality Job Descriptions and Person Specs in timely fashion • Apply lean principles (Value Stream Analysis) to recruitment process • Database of approved interviewers • Employ scoring matrix to interviewees • Improved use of assessment testing • Conduct ‘block’ interviews • What innovation is required (if any)? • Is anyone doing it already? • Are there additional effects on the system? Barts and the Royal London • Expect reduction in turnover of new appointees • Reduction in bank & agency usage will improve quality of care. * QIPP = Quality, innovation, productivity, and prevention ** Initiatives should be quality-neutral or have a positive impact on quality CONFIDENTIAL AND PROPRIETARY Any use of this material without specific permission of McKinsey & Company is strictly prohibited
Template for QIPP Ideas Headline / Title: Establish an effective & efficient treatment journey for Stroke patients Short description: Care for Stroke patients can be improved by expedient admission to a dedicated Stroke Unit (CQUIN target 4 hours), having extensive time on the Stroke Unit (CQUIN target 90% of their hospital stay), proactive, goal-oriented Multi-Disciplinary Team (MDT) assessments linked to the community and criteria led discharge planning. QIPP elements* Making it happen Achievement of CQUIN targets (increase admission to Stroke Unit in 4 hours from 0% to 75%, increase proportion of patients which spend 90% of their time on Stroke Unit from 70% to 75%) • Availability & suitability of community facilities to support discharge • Ability to maintain operating policy out of hours • Ability to change daily schedule (visiting times, staff breaks) • Estimated quality impact** • What are the main barriers for implementation? • Estimated productivity impact Reduce average Length of Stay (LoS) from 19 to 14 days • Support from Executive Team • Team to develop ‘as is’ & ‘to be’ processes • Specification of ‘Key Worker’ role • Stroke Unit operational policy (inc. criteria led discharge) • Admission & Triage to Stroke Unit incl. Assessment area • What needs to be in place in order to implement? • Is it linked to the prevention agenda (if at all)? No • What clinical engagement will be required? • Engagement & direction throughout process redesign of: • Stroke consultants • all Multi Disciplinary Team (MDT) specialties • Emergency Stroke Outreach Team (ESOT) • Apply lean principles (Value Stream Analysis, Rapid Improvement Events) to Stroke patient journey • Establish Emergency Assessment Area on Stroke Unit • Co-locate MDT’s on Stroke Unit • Incorporate Productive Ward methodology • Implement Key Worker role • What innovation is required (if any)? • Is anyone doing it already? • Improvements to ward hand-over processes • Community team involvement accelerates discharge • Clarity of patient communications and improvement in patient satisfaction • Are there additional effects on the system? No * QIPP = Quality, innovation, productivity, and prevention ** Initiatives should be quality-neutral or have a positive impact on quality CONFIDENTIAL AND PROPRIETARY Any use of this material without specific permission of McKinsey & Company is strictly prohibited
Template for QIPP Ideas Headline / Title: Establish an integrated and robust patient flow pathway for Rehabilitation and Discharge Short description: Apply lean principles to the patient journey to define a pathway covering their rehabilitation and discharge in which each MDT member has clear roles and responsibilities, staff are empowered in the decision making process, dedicated Rehabilitation & Discharge areas are occupied by appropriate patients, and Length of Stay is minimised. QIPP elements* Making it happen • Increase proportion of suitable patients on Rehab / Discharge areas from 33% to 100% to provide specialist care • Provide 95% of patients with an MDT assessment within 12 hrs of admission • Financial investment & commitment required • Physical changes to configuration of wards • Availability of community facilities for patients suitable for discharge • Implementing new admissions policy and Unified Rehabilitation Process (URP) across the Trust • Estimated quality impact** • What are the main barriers for implementation? • Estimated productivity impact Reduce average Length of Stay (LoS) in Rehab ward from 25 to 15 days Reduce number of patient beds by 12 • What needs to be in place in order to implement? • Support from Executive team • Team to develop ‘as is’ & ‘to be’ processes • Rehab Integrated Care Plan (ICP) • (Goal driven) Criteria led discharge policy • Is it linked to the prevention agenda (if at all)? No • Engagement & direction throughout process redesign of: • Ward consultants, managers & staff • All Multi Disciplinary Team (MDT) specialties • Bed Managers, Patient Flow & discharge teams • What clinical engagement will be required? • Apply lean principles (Value Stream Analysis) to Rehab & Discharge pathways • Establish combined Rehab / Discharge area operating single sex sleeping areas • Clear admission/discharge criteria with a clear process for referral • What innovation is required (if any)? • Is anyone doing it already? • Combined wards require fewer stock types and overall less local stock holding • Improved awareness of & focus upon needs of patients nearing discharge • Improvement in patient experience • Are there additional effects on the system? No * QIPP = Quality, innovation, productivity, and prevention ** Initiatives should be quality-neutral or have a positive impact on quality CONFIDENTIAL AND PROPRIETARY Any use of this material without specific permission of McKinsey & Company is strictly prohibited