Download
1 / 18
180 likes | 239 Views
Learn about the intricate mechanisms of blood pressure regulation, including chronic and acute factors, and explore the causes and management of resistant hypertension. Discover key points for diagnosing and treating secondary hypertension, adrenal incidentaloma, and hormonal imbalances affecting blood pressure control.

E N D
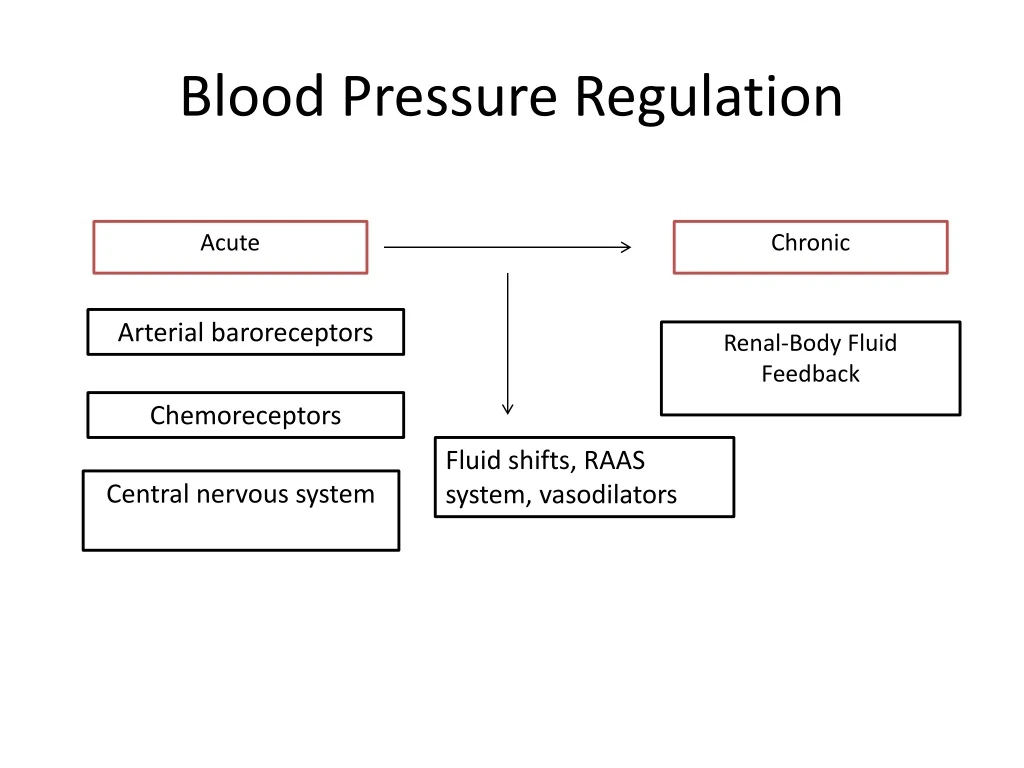
Blood Pressure Regulation Chronic Acute Arterial baroreceptors Renal-Body Fluid Feedback Chemoreceptors Fluid shifts, RAAS system, vasodilators Central nervous system
Secondary Hypertension Hyperaldosteronism Hypokalemia Pheochromocytoma Flushing not pallor with spells Cushing’s Weight gain, fatigue, bruising.. syndrome Hypothyroidism Volume changes -> increased renin Intracellular calcium -> aldosterone? Hyperparathyroidism SNS, oxidative stress to endothelium Sleep apnea Blood pressure upper vs lower variable Coarctation of aorta Salt and water retention, hormonal Renal disease
Resistant Hypertension Systolic blood pressure ≥ 140 or diastolic blood pressure ≥ 90 on 3 or more antihypertensives and 1 must be a diuretic. OR Blood pressure is controlled but requiring ≥ 4 antihypertensives
Resistant Hypertension • Lifestyle and diet (excessive salt intake, excessive alcohol intake) • Suboptimal antihypertensive choice (some groups argue the 3 agents must include not only a diuretic but also an ACEi/ARB and a CCB) • Suboptimal antihypertensive dose • Medications (NSAIDs, ASA, decongestants, diet pills) • Stimulants (prescription or illegal) • Obesity • Oral contraceptives
Resistant Hypertension Treatment BP >140/90 on 3 meds Secondary causes ruled out or treatment of did not correct BP Serum K+ If failing these measures consider alpha blockers, beta blockers, switching to loop diuretics <4.5 >4.5 Add spironolactone Double thiazide dose
Which of the following tests would you order in this patient with a newly identified adrenal mass? • 1 mg overnight dexamethasone suppression test • 24 hour urine metanephrines and catecholamines • 24 hour urinary aldosterone excretion test • A and B • All of the above
Adrenal Incidentaloma • A mass > 1 cm that is discovered incidentally by radiologic examination • There are two questions that should be answered with evaluation: • Is it malignant? • Is it functioning?
Is it malignant? • The maximum diameter of the adrenal mass is predictive of malignancy • Suspect if > 6 cm (some studies say > 4 cm) • Radiographic characteristics and change in size over time also have strong predictive value
Is it functioning? If you know what hormones each layer of the adrenal gland produces, you can determine what tests to order to see if the incidentaloma is functioning “GFR”
Is it functioning? “GFR” Mineralocorticoids Glucocorticoids Androgens Catecholamines “Salt, sugar, sex: the deeper you go, the sweeter it gets”
Is it functioning? Mineralo-corticoids “GFR” Aldosterone Glucocorticoids Cortisol Androgens DHEAS Epinephrine Norepinephrine Catecholamines
Is it functioning? Too much aldosterone? CONSIDER Primary hyperaldosteronism G Too much cortisol? Cushing’s syndrome CONSIDER F Adrenocortical carcinoma Too much DHEAS? CONSIDER R Too much catecholamines? CONSIDER Pheochromocytoma
“GFR” Is it functioning? Plasma aldosterone and renin ratio Too much aldosterone? ORDER Primary hyper-aldosteronism CONSIDER 1 mg overnight dexamethasone suppression test ORDER Cushing’s syndrome CONSIDER Too much cortisol? ORDER Serum DHEAS, imaging Adrenocortical carcinoma CONSIDER Too much DHEAS? 24 hour urine metanephrines and catecholamines Pheochromo-cytoma ORDER Too much catecholamine? CONSIDER
‘Is it functioning?’: Diagnosis • All asymptomatic patients with adrenal incidentaloma should have: • 1 mg overnight dexamethasone suppression test • 24-hour urine levels of metanephrines and catecholamines • If patients have hypertension or spontaneous hypokalemia: • Also order plasma aldosterone-plasma renin ratio
‘Is it functioning?’: Diagnosis Pearls • Overnight dexamethasone test should be done if subclinical Cushing’s syndrome • If signs of Cushing’s syndrome, order 24-hour urinary free cortisol instead (more specific) • Any situation (i.e. illness requiring hospitalization) or medication (i.e. TCA) that increases endogenous production of catecholamines can lead to a false positive fractionated metanephrines and catecholamines result • Cannot measure plasma aldosterone concentration in patients on spironolactone, eplerenone, or high-dose amiloride
Management • Incidentaloma > 6 cm, malignant, or functioning: • Surgical removal • Incidentaloma 4 – 6 cm: • Controversy regarding management • Incidentaloma < 4 cm and non-functioning: • Monitored radiographically (repeat imaging in 6-12 months)
Teaching Points • When working up difficult to control blood pressure remember to use physical exam findings and symptoms to rule out underlying diseases contributing. • When you find an adrenal incidentaloma you need to ask yourself two questions: is it malignant? Is it functioning? • Once you have determined an incidentaloma is not malignant and non-functioning management depends on size of the nodule.