Download
1 / 14
140 likes | 526 Views
Oct. 14. Oct. 19 upright. Oct. 19 supine. Oct. 19. Morning Report. Anne Lachiewicz November 20, 2009. Malar rash Discoid rash Photosensitivity Oral/nasopharyngeal ulcers Nonerosive arthritis Serositis Proteinuria or urinary cellular casts Seizures or psychosis

E N D
Oct. 19 upright
Oct. 19 supine
Morning Report Anne Lachiewicz November 20, 2009
Malar rash Discoid rash Photosensitivity Oral/nasopharyngeal ulcers Nonerosive arthritis Serositis Proteinuria or urinary cellular casts Seizures or psychosis Hemolytic anemia or leukopenia or lymphopenia or thrombocytopenia + ANA + anti-ds-DNA, anti-sm, or antiphospholipid Abs Am Coll. Rheum. Classification Criteria for SLE (if >= 4/11, Se & Sp >95%)
SLEDAI (SLE Disease Activity Index) • Created to standardize outcomes measures in SLE • A "weighted" index of 9 organ systems for disease activity in SLE: • 8 for central nervous system and vascular • 4 for renal and musculoskeletal • 2 for serosal, dermal, immunologic • 1 for constitutional and hematologic • Maximum theoretical score is 105, but few patients have scores greater than 45 • Scores < 10 mild, 10-20 moderate, >20 severe • Validated
GI manifestations (30%)Not included in classification criteria or in the disease activity index) • Dysphagia (25-40%) – usually due to esophageal hypomotility • Abdominal pain with N/V (30%) – many reasons, consider SLE meds (steriods, azathi0prine) • Peritonitis (60-70% lifetime) • Ascites (uncommon)
GI manifestations • Peptic ulcer disease (11-50%) - usually gastric, ? SLE meds (NSAIDS, steriods) vs. SLE itself • Pancreatitis (2-8%, may be more common) *can see elevated amylase in SLE w/o pancreatitis • Liver disease - hepatomegaly & abnormal liver tests are common, but ESLD is rare • Protein-losing enteropathy – small series/case reports, young women, 50% have diarrhea
Mesenteric vasculitis & infarction (lupus enteritis) • Vasculitis of the small arterial vessels or venules • ? More frequent in young women early in the course of SLE • ? Correlation with SLEDAI • Colicky lower abdominal pain • Generally insidious & may be present for months prior to acute abdomen • Potentially life-threatening – bowel necrosis, perforation, sepsis, hemorrhage • M&M has improved due to early recognition & treatment (more CT scans)
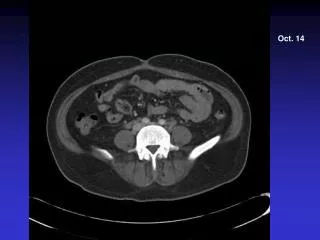
Lupus enteritis: Diagnosis • No established diagnostic criteria • Most commonly in jejunum & ileum, rectal involvement is rare • May be focal or diffuse (involving several vascular territories) • CT scan: ascites with peritoneal enhancement, bowel walk thickening, dilated bowel loops & prominence of mesenteric vessels with palisade pattern or comb-like appearance • Not associated with any specific antibodies, but relapse may be more common in those with APLA
Lupus enteritis: Treament • NPO, NG tube, IVF/TPN • Blood cultures, r/o infection • Consult surgery • IV methylprednisolone + cyclophosphamide • Check lactate & abdominal films regularly as steriods may mask peritonitis
References • Kwok S-K, Seo S-H, et al. Lupus enteritis: clinical characteristics, risk factor for relapse and association with anti-endothelial cell antibody. Lupus 2007; 16:803-809. • Lee C-K, Ahn MS, et al. Acute abdominal pain in systemic lupus eythematosus: focus on lupus enteritis (gastrointestinal vasculitis). Ann Rheum Dis 2002; 61:546-550. • Lian T-Y, Edwards CJ, et al. Reversible acute gastrointestinal syndrome associated with active systemic lupus erythematosus in patients admitted to hospital. Lupus 2003; 12:612-616. • Massarotti EM, Schur PH. Gastrointestinal manifestations of systemic lupus erythematosus. In: UpToDate, Basow, DS (Ed), UpToDate, Waltham, MA, 2009. • Vegara-Fernandez O, Zeron-Medina J, et al. Acute abdominal pain in patients with systemic lupus erythematosus. J Gastrointest Surg 2009; 13:1351-1357.