Download
1 / 28
280 likes | 374 Views
This presentation outlines the NYS Health Home program, focusing on care management history, objectives, policy goals, and the importance of Health Homes in addressing complex healthcare needs. It also covers provider qualification standards, payment methodology, and care integration/coordination.

E N D
NYS Health Home Program Presentation to the National Academy for State Health Policy June 14, 2012
View from New York • Many of the over five million Medicaid enrollees are relatively healthy and obtain only episodic & preventive healthcare. • However, several population groups contain complex medical, behavioral and long term care needs and have difficulty navigating the system. • The high need members drive up high cost services including inpatient & long term institutional care. 2
Care Management History in NY • Other care management initiatives are disease specific Targeted Case Management (TCM) – Mental Health AIDS/COBRA - for HIV+ individuals Managed Addiction Treatment Services (MATS). • During 2009, New York funded six FFS Chronic Illness Demonstration Projects to provide care coordination for individuals exempt or excluded from mandatory managed care. • Governor Cuomo’s vision for Medicaid reform is care management for all. • The MRT recommended Health Homes as one of 79 recommendations. 3
NYS Objectives • Primary goal: Comprehensively address the complex needs of Medicaid beneficiaries who qualify for Health Home services including: • Physical (primary care physicians & prevention) • Behavioral (mental illness & chemical dependency) • Social (such as housing and entitlement programs) 4
New York State’s 3-4 top policy objectives for Health Homes • Effectively manage the health, behavioral health and long term care needs of complex, high-cost populations. • Breakdown traditional silos in care delivery and create partnerships that shape a more coordinated health care delivery system. • Align incentives with quality and cost effectiveness. • Bend the cost curve. 5
Why Health Homes? • Engaging and managing services for members with complex chronic conditions is essential in controlling future health care costs. • Section 2703 provides a new funding opportunity to better provide coordinated services. • Health Homes are expected to reduce costs while improving outcomes & patient satisfaction. 6
Complex Populations: All Ages Total Complex N =1,050,385 $2,366 PMPM 32% Dual 55% MMC $28.2 Billion 7 Time Period: July 1, 2010 – June 30, 2011
NYS Medicaid Beneficiaries with Multiple Chronic Illnesses 8
Health Home Infrastructure • Health Homes include designated providers working with multidisciplinary partners. • Provider qualification standards were developed working with hospitals, clinics, physicians, mental health experts, chemical dependency experts & housing providers, as well as other state agencies. • Care managers will lead multidisciplinary teams to assure member needs are met. 10
Provider Qualification Standards General Qualifications • Must be enrolled (or be eligible for enrollment) in the NYS Medicaid program and agree to complywith all Medicaid program requirements. • Can either directly provide, or subcontract for the provision of, health home services. Responsible for all health home program requirements, including services performed by the subcontractor. 11
Provider Qualification Standards General Qualifications (continued) • Care coordination and integration of heath care services will be provided to all health home enrollees by an interdisciplinary team of providers, where each individual’s care is under the direction of a dedicated care manager who is accountable for assuring access to medical and behavioral health care services and community social supports as defined in the enrollee care management plan. • Must meet standards for delivery of six core health home services as described in following slides. Must provide written documentation that clearly demonstrates how the requirements are being met. 12
Provider Qualification Standards Health home providers will be required to followFederal and State requirements for Health Homes: • Comprehensive care management; • Care coordination and health promotion; • Comprehensive transitional care; • Patient and family support; • Referral to community and social support services; • Use of health information technology (HIT) when feasible. 13
Payment Methodology • Payment is made on a PMPM basis in two increments: • Outreach & Engagement • Delivery of Active Care Coordination • HH bills NYS directly for FFS members and then funnel payments as appropriate to partner. • TCMs, MATS & CIDPs bill directly to State. • Managed Care Plans keep up to 3% for administrative services and pay the lead HH. 14
Care Integration/Coordination • Health Homes are not held to specific models but will be held to meeting quality standards. • Each Health Home has partners that can meet both physical and behavioral health needs. • Care Coordinators are responsible for managing the whole person not specific conditions. • Health Homes are held responsible for meeting quality not process measures. 15
Health Home Services • Health home providers will be required to provide the following health home services in accordance with federal and State requirements: • Comprehensive care management • An individualized patient centered care plan based on a comprehensive health risk assessment – must meet physical, mental health, chemical dependency and social service needs. • Care coordination and health promotion • One care manager will ensure that the care plan is followed by coordinating and arranging for the provision of services, supporting adherence to treatment recommendations, and monitoring and evaluating the enrollee’s needs. The health home provider will promote evidence based wellness and prevention by linking patient enrollees with resources for smoking cessation, diabetes, asthma, hypertension, self-help recovery resources, and other services based on need and patient preference. • Comprehensive transitional care • Prevention of avoidable readmissions to inpatient facilities and oversight of proper and timely follow-up care. 16
Health Home Services (cont’d) • Patient and family support • Individualized care plan must be shared with patient enrollee and family members or other caregivers. Patient and family preferences are considered. • Referral to community and social support services • Provider will identify and coordinate community and social supports • Use of health information technology (HIT) when feasible • Health home providers will be encouraged to utilize RHIOs or a qualified entity to access patient data and to develop partnerships that maximize the use of HIT across providers. Health home provider applicants must submit a plan with their application for achieving compliance with the final health home HIT requirements within 18 months of program implementation 17
Health Information Technology • Initial standards must be met at start-up: • Structured information systems, policies, procedures & practices for individual plans of care; • Systematic process to follow-up on tests, treatments, services and referrals; • Have health record system to allow PHI and plan of care accessible to interdisciplinary team for management & analysis; • Make use of available HIT and access member data thru RHIO or QE to conduct all processes. • Providers have 18 months to achieve final standards in SPA. 18
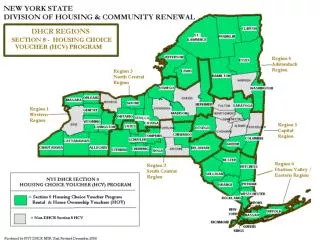
Program Status • To date there are 34 designated Health Homes: • Phase 1 encompasses 10 counties with 13 HH; • Phase 2 contains 13 counties with 21 HH; • Phase 3, not yet designated, will serve 39 counties. • Of the almost one million eligible members, about 6,000 members are either in Outreach and Engagement or active Care Management. • NYS is working closely with Plans and Health Homes. 20
How Eligible Members are Being Identified and Assigned • New York State Health Home Analytical Products • CRG Based Attribution– For Cohort Selection • CRG Based Acuity – For Payment Tiers • Predictive Model - Predicts future negative events (Inpatient, Nursing Home, Death) using claims and encounters – For Assignment Priority • Ambulatory Connectivity Measure – For Assignment Priority • Provider Loyalty Model – Establishes Patient Connectivity to Existing Care Management, Ambulatory (including BH), ED and Inpatient – For Matching to Appropriate HH and to Guide Outreach activity. 21
Monthly Care Management Tracking Elements • Patient Demographic information, Health Plan • Assigned Health Home, Health Home Care Management Provider • TCM, COBRA, MATS, CIDP, MCO, CBO • Enrollment/Disenrollment Status, Various Dates • Consent • Enrollment/disenrollment • Patient Profile (e.g., Risk Score, Acuity Score, Ambulatory Connectivity and Loyalty) 22
Functional Assessment • NYS is evaluating a functional self-assessment tool based on the FACT-GP to assess each Health Home participant on a range of measures. Please see: http://www.health.ny.gov/health_care/medicaid/program/medicaid_health_homes/forms/ • Validated tool administered face-to-face upon enrollment, annually thereafter and at discharge; results are reported to the State. • Results of assessments used to adjust initial rates, which were based on calculated acuity and risk scores. 24
Cost Saving Estimates • Initial Savings to come from converting current care management programs. • Estimated savings are @ $40 million this FY. • Long term savings must come from quality of care improvements: • Reduction in ER utilization and Hospitalization; • Reduction in nursing home admissions; • Effective primary care utilization. 25
Barriers/Challenges • FFS Member Lists • Finding people - DIFFICULT • Contracts with Plans • Guidance to Converting • Community Referrals • Medicare/Medicaid Gainsharing 26
Successes/Lessons Learned • Proudest achievements: • Offered an opportunity for direct care providers and community-based organizations to partner • Opportunity to improve communications • Advice for other states in planning stages or thinking about pursuing 2703: • Include providers and plans on development • Communication with all stakeholders • Administrative functions and resources • In hindsight, what would you have done differently? • Include Managed Care Plans earlier in process 27
Need More Information? Have Questions/Comments? • NYS Health Home Web site (links to many relevant materials including accessing applications): http://nyhealth.gov/health_care/medicaid/program/medicaid_health_homes/index.htm. • Questions and/or comments regarding New York's implementation of Health Homes can be directed to hh2011@health.state.ny.us. 28