Download
1 / 65
700 likes | 1.04k Views
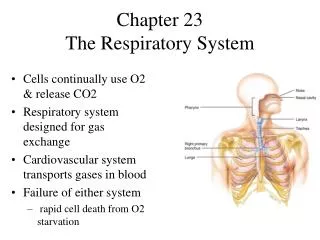
Respiratory: Respiratory Failure and ARDS. Marnie Quick, RN, MSN, CNRN. Normal Respirations: Tidal Vol; Inspiratory & Expiratory reserve Vol; Residual Vol; Vital Capacity; Anatomical dead space. Normal gas exchange in lung. Blood Supply to Lung. Respiratory Failure.

E N D
Respiratory: Respiratory Failure and ARDS Marnie Quick, RN, MSN, CNRN
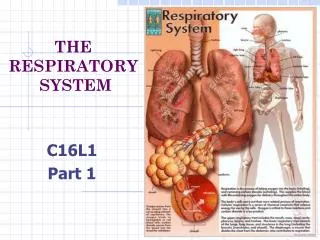
Normal Respirations: Tidal Vol; Inspiratory & Expiratory reserve Vol; Residual Vol; Vital Capacity; Anatomical dead space
Respiratory Failure • Not a disease process, sign of severe dysfunction • Results when one or both gas exchanging systems inadequate; atmosphere (to lung) or blood • Alveolar ventilation inadeq to meet body’s need • Commonly defined in terms of ABG’s: • PO2 of less than 50 mmHg • PCO2 greater than 50 mmHg • Arterial pH of less than 7.35
Predisposing factors for Resp Failure: Airways/alveoli; CNS; Chest Wall; Neuromuscular- Table in Lewis p 1801 Most common cause: COPD
Hypoxemic Respiratory Failure • Oxygenation failure- inadequate O2 transfer between alveoli & pulmonary capillary bed • PaO2: 60 mm Hg or less on 60 % O2 • Inadequate O2 saturation of hemoglobin • Causes tissue hypoxia> Metabolic acidosis; cell death; decreased CO; impaired renal function • Common causes: disorders that interfere with O2 transfer into the blood- respiratory or cardiac system (Lewis p. 1800 Table 68-1)
Hypoxemic Respiratory Failure Mechanisms that may lead to Hypoxemia: 1. Mismatch ventilation & perfusion (V/Q mismatch) • V/Q: Volume blood perfusing lungs each minute • Each ml of air for each ml of blood • 1:1= V/Q ratio of 1 • Causes of V/Q mismatch: • Ventilation portion blocked (secretions in airway/alveoli, airway/alveolar collapse, decreased movement chest/ventilation) • Perfusion portion blocked (pulmonary embolus) • Treat: O2(reverse hypoxemia); treat cause
Hypoxemic Respiratory FailureRange of ventilation to perfusion (V/Q relationship) • A. Absolute shunt, no ventilation fluid in alveoli • B. Ventilation partially compromised- secretions • C. Normal lung unit • D. perfusion partially compromised by emboli obstructing blood flow • E. Dead space: no perfusion- obstruction of pulmonary capillary
Hypoxemic Respiratory FailureMechanisms that may lead to Hypoxemia: 2. Shunt- Extreme V/Q mismatch • Occurs when blood leaves heart without gas exchange • Types: • 1. anatomic shunt: blood does not pass through lungs • 2. intrapulmonary shunt- alveoli fill with fluid • Treatment: Mechanical ventilation to force O2 into lungs; treat cause
Hypoxemic Respiratory FailureMechanisms may lead to Hypoxemia: 3. Diffusion limitations • Alveoli membrane thickened or destroyed • Gas exchange across alveolar-capillary membrane can’t occur • Classic sign: hypoxemia present during exercise, not at rest • Treat the cause- pulmonary fibrosis; ARDS
Hypoxemic Respiratory FailureMechanisms may lead to Hypoxemia: Clinical Manifestations of Hypoxemia • Specific: Respiratory: • Dyspnea; tachypnea; prolonged expiration; intercostal muscle retraction; use of accessory muscles in resp;< 80% SpO2; paradoxic chest/abd wall movement with resp cycle (late); cyanosis (late) • Nonspecific: • Cerebral: agitation, disorientation, delirium, restless, combative, confusion, dec LOC, coma (late) • Cardiac: tachycardia, hypertension, skin cool/clammy, dysrhythmias (late), hypotension (late) • Other: fatigue; need to pause to breath when speaking
Hypercapnic Respiratory Failure • Ventilatory failure with insufficient CO2 removal • PaCO2 greater than 45 mm Hg • Arterial pH less than 7.35 • PCO2 rises rapidly and respiratory acidosis develops: PO2 drops more slowly • Common causes: disorders that compromise lung ventilation and CO2 removal (Lewis Table 68-1)
Hypercapic Respiratory Failure • Ventatory failure: Inability of the respiratory system to ventilate out sufficient CO2 to maintain normal PaCO2 • Specific Causes: • Airways/alveoli: asthma, COPD, cystic fibrosis • CNS: drug overdose- depressant, brainstem dysfuction, metabolic causing decreased LOC; high SCI injuries- decrease/absent diaphragm/chest movement • Chest wall: pain, flail chest, rib fractures, mechanical restriction, kyphoscoliosis, obesity • Neuromuscular: resp muscles weak/paralysis- MS, MG, MD, Guilain-Barre Syndrome
Hypercapic Respiratory Failure Clinical Manifestations • Specific: • Respiratory: Dyspnea; dec resp rate or rapid with shallow resp; dec tidal vol; dec min ventilation • Nonspecific: • Cerebral: AM headache; disorientation, progressive sommolence; coma (late) • Cardiac: dyshythmias; hypertension; tachycardia; bounding pulse • Neuromuscular: muscle weakness; dec deep tendon reflexes; Tremor/seizures (late)
Collaborative Care for Respiratory Failure: Diagnostic tests • History/physical assessment • Pulse oximetry • ABG analysis • Chest X-ray • CBC, sputum/blood cultures, electrolytes • EKG • Urinalysis • V/Q scan- if pulmonary embolism suspected • Hemodynamic monitor/pulmonary function tests
Collaborative care for Respiratory Failure Respiratory Therapy • Main treatment- correct underlying cause & restore adequate gas exchange in lung • Elevate HOB • Oxygen Therapy • Maintain PaO2 at least 60 mm Hg • SaO2 at least 90% • Mobilization of secretions • Hydration & humidification • Chest physical therapy • Airway suctioning • Effective coughing & positioning • Positive pressure ventilation • Noninvasive positive pressure ventilation • Intubation with mechanical ventilation
Collaborative Care for Respiratory Failure cont • Drug Therapy • Relief bronchospasm; reduce airway inflam and pulmonary congestion; treat pulmonary infections; reduce anxiety, pain • Medical supportive therapy • Treat underlying cause • Nutritional therapy • Enteral; parenteral • Protein and energy stores
Collaborative Care: Artifical airways- tracheostomy and endotracheal tubes
Suctioning with closed (inline) suctioning-used with tracheostomy or endotrach tubes
Complications of endotracheal intubation • 1. Extubation • Restraints • 2. Aspiration • Tube at right allows for subglottal suctioning
Collaborative Care: Mechanical Ventilation • Provide adeq gas exchange • Types- Positive, Neg • Settings- Table 66-11 • Modes- Table 66-12 • Criteria to put on vent • RR > 35-45 • pCO2 >45 • pO2 <50
Types: Positive pressure mechanical ventilation with endotracheal tube (PPV)
Types: Positive pressure- Noninvasive (tight fitting mask) positive pressure ventilation (CPAP)
Alarm settings • Assess your patient – not the alarm!!!!! • Never turn alarms off • Alarms sound when you have low pressure or high pressure in the ventilator • Note “alarm silence” and “alarm reset” on picture to the right
Low Pressure • Circuit leaks • Airway leaks • Chest tube leaks • Patient disconnect from vent or tube • High Pressure • Patient coughing • Secretions or mucus in the airway • Patient biting tube • Airway problems • Reduced lung compliance (as a pneumothorax) • Patient fighting the ventilator • Accumulation of water in the tube • Kinking of tube
Modes of PPV • Volume Ventilation • Predetermined tidal volume (TV) is delivered with each inspiration • Tidal volume (TV) is consistent, airway pressures will vary • Pressure Ventilation • Predetermined peak inspiratory pressure • Tidal volume (TV) will vary, airway pressures will be consistent
Ventilator settings of Modes (Table 66-12 p.1761) • Volume Modes • CMV; AC; SIMV • Predetermined tidal volume (TV) is delivered with each inspiration • Tidal volume (TV) is consistent, airway pressures will vary • Pressure Modes • PSV; PC-IRV • Predetermined peak inspiratory pressure • Tidal volume (TV) will vary, airway pressures will be consistent • Other Modes • PEEP and CPAP
Ventilator settings- Other modes • Positive End-Expiratory Pressure • Positive pressure is maintained at the end of expiration • Pressure at end expiration keeps alveoli from collapsing, improving functional residual capacity (FRC) • Used with other modes on the ventilator • Purpose is to improve oxygenation while limiting risk of O2 toxicity • Used to treat ARDS
Ventilator settings- other modes • Continuous Positive Airway • Similar to PEEP • However, pressure in CPAP is delivered continuously • Prevents airway pressure from falling to zero • Measured in cm H20 • Can be administered noninvasively (by mask) or through ETube or TTube • Used in treatment of obstructive sleep apnea
Complications of Positive Pressure Mechanical ventilation • Cardiovascular: decreased CO; inc intrathoracic pressure • Pulmonary: Barotrauma; Volutrauma; alveolar hypoventilation/hyperventilation; ventilator-associated pneumonia • Sodium and water imbalance • Neurological: impaired cerebral bl flow>IICP • Gastrointestional: stress ulcer/GI bleed; gas; constipation • Musculoskeletal: dec muscle tone; contractures; footdrop; pressure ulcers from BR • Psychosocial: physical & emotional stress; fight vent
Nursing Care for complications • Neurological – elevate head of bed, keep body in proper alignment • Respiratory – monitor cuff inflation, vent settings, ABG’s, for hyperventilation, hypoxemia • Cardiovascular – monitor NIBP and arterial pressures, CO, capillary refill, HR & rhythm • Gastrointestinal – set up schedule for BM, admin laxatives, PPI, admin tube feedings • Musculoskeletal – passive & active ROM, turn q2h, keep body in proper alignment
Other problems when on mechanical ventilation • Machine disconnection or malfunction • Nutrition needs • Weaning from ventilator/ extubation • Spontanenous breathing trial (SBT) Hospital protocol • Document progress • Table 66-13 p.1767- readiness/assessment
Exhaled C02 (ETC02) normal 35-45 Used when trying to wean patient from a ventilator
Nursing assessment specific to Respiratory Failure • Assess both airway and lungs- note picture to right • Refer to hypoxic and hypercapnic respiratory failure symptoms • Table 68-4 p. 1806 • Subjective data • Objective data
Relevant Nursing Problems related to Respiratory Failure • Prevention of acute respiratory failure • Nursing Care Plans (p.1807-09) • Gerontology considerations • Nursing Care Plans Mechanical ventilation (NCP 66-1 p.1754) • Suctioning procedure and oral care (p.1757-8)
Acute Respiratory Distress Syndrome ARDS • Sudden progressive form of acute respiratory failure • Alveolar capillary membrane becomes damaged and more permeable to intravascular fluid • Results in noncardiac pulmonary edema and progressive refractory hypoxemia • ARDS is NOT primary! • Follows various pulmonary or systemic conditions • Sepsis is the most common cause