Download
1 / 57
570 likes | 695 Views
Chronic Obstructive Pulmonary Disease. Naima Cheema, MD Emory Family Medicine March 20, 2008. Agenda. COPD Introduction Journal Introduction Background & Hypothesis Study Design Study Population Demographics Mortality Analysis Efficacy Analysis Summary. Agenda. COPD Introduction

E N D
Chronic Obstructive Pulmonary Disease Naima Cheema, MD Emory Family Medicine March 20, 2008
Agenda • COPD Introduction • Journal Introduction • Background & Hypothesis • Study Design • Study Population • Demographics • Mortality Analysis • Efficacy Analysis • Summary
Agenda • COPD Introduction • Journal Introduction • Background & Hypothesis • Study Design • Study Population • Demographics • Mortality Analysis • Efficacy Analysis • Summary
COPD • Chronic pulmonary inflammation characterized by partial or irreversible airway obstruction • Two types • Chronic bronchitis • Emphysema • Clinical Findings • Present in 5th or 6th decade of life • Excessive cough • Sputum production • Shortness of Breath
COPD • Lab Findings • Spirometry – Decreased FEV1, FVC and FEV1/FVC • <10% reversibility post bronchodilation therapy • Increase RV, TLC and RV/TLC
Treatment • Smoking cessation • Oxygen if resting PaO2 < 55mmHg or SO2 < 88% • Bronchodilators • Inhaled steroids • Methyl Xanthine • Oral steroids
Acute Exacerbations of COPD • Clinical Findings • Increased sputum production • Increased purulence of sputum • Increased dyspnea
Common Causes of COPD exacerbations • Mild to moderate exacerbations • Streptococcus pneumoniae • Haemophilus influenzae • Moraxella catarrhalis • Chlamydia pneumoniae • Mycoplasma pneumoniae • Viruses • Severe exacerbations • Pseudomonas species • Other gram-negative enteric bacilli
Treatment • Bronchodilators • Antibiotics • Systemic steroids • Methyl Xanthine • Health maintenance • Pneumovax every 5 yrs • Influenza vaccine yearly
Management of COPD Inhaled Steroid
Agenda • COPD Introduction • Journal Introduction • Background & Hypothesis • Study Design • Study Population • Demographics • Mortality Analysis • Efficacy Analysis • Summary
Journal Introduction • Name • TORCH Trial (Towards a Revolution in COPD Health) • Title • Salmeterol and Fluticasone Propionate and Survival in COPD. • Authors • Calverly P, Anderson J, Celli B, Ferguson G, et al. • Published • New England Journal of Medicine, Feburary 22,2007, Vol.356:775-789 • Sponsor: • GlaxoSmithKline • Type: • Therapeutic Trial
Agenda • COPD Introduction • Journal Introduction • Background & Hypothesis • Study Design • Study Population • Demographics • Mortality Analysis • Efficacy Analysis • Summary
Background • COPD is an inflammatory condition of lungs. • Major cause of illness, death and use of healthcare resources worldwide. • COPD causes approx. 2.5 million deaths annually. • Current treatment of COPD minimizes risk factors, improves symptoms and prevents exacerbations with little focus on improving survival • No treatment has been shown to reduce mortality
Background • Survival in COPD has improved with • Smoking cessation in early disease • Home oxygen for persistent hypoxemia • Lung reduction surgery in selected pt. with emphysema. • Inhaled corticosteroids reduce frequency of exacerbations especially when combined with inhaled LABA. • Retrospective analysis suggest that inhaled corticosteroids reduce mortality rate among pt. with COPD and adding LABA may augment this effect.
Hypothesis • Combination of long acting beta agonist salmeterol and inhaled corticosteroid fluticasone propionate would reduce mortality among pt. with COPD.
Agenda • COPD Introduction • Journal Introduction • Background & Hypothesis • Study Design • Study Population • Demographics • Mortality Analysis • Efficacy Analysis • Summary
Study Design • Placebo controlled, Double blind, Randomized, Parallel group trial • Conducted in 444 centers in 42 countries • 6200 Patients with moderate to severe COPD • Pts. were divided into 4 groups. • Salmetrol + Fluticasone propionate - Advair, Seretide • Placebo • Salmeterol alone - Serevent • Fluticasone Propionate alone – Flovent, Flixotide • All medicines used in study are manufactured by GalaxoSmithKlein.
Study Design • 2 wks of run-in period, 3 yr treatment phase, 2 wks followup phase
Study Design • Two arms of the trial • Efficacy arm • Safety arm • Efficacy Arm • Primary Outcome: Death from any cause • Secondary Outcome: • Decreased Frequency of exacerbations • Improved Health Status • Improved Spirometry • Safety Arm • Adverse Events • Bone Fractures • Cataracts
Study Design • Secondary End Point: • Frequency of exacerbations : • Defined as symptomatic deterioration requiring treatment with antibiotics , systemic steroids, or hospitalization . • Health Status : • Assessed according to scores on St. George’s Respiratory Questionnaires. Scores from 0-100. • A change of 4 units is considered clinically relevant • The questionnaire was administered in 28 countries where validated translations were available.
Study Design • Secondary End Point (Contd.) • Lung Functions: • Assessed with use of post bronchodilator spirometery • For pt. who withdrew from study, all data available at the time of withdrawal was included
Study Design • All medicines are taken in the morning and evening for 3 yrs. • Meds. were administered as dry powder with the use of inhaler (diskus, accuhaler by GSK). • Inhalers were collected every 12 wks. • No. of doses in each inhaler were recorded to check adherence to study regimen. • Before the run in period , use of all corticosteroids and inhaled LABA was stopped, but pt. could continue other meds. for COPD.
Study Design • Safety Evaluation • Common adverse effects with steroid use include fractures and cataract • Adverse events were reviewed at each visit. • Information was collected about any fracture; traumatic or non-traumatic. • Non-traumatic fracture was considered when it occurred as a result of spontaneous fall or fall from less than standing height. • A safety substudy was conducted in USA only involving 658 pt. • DEXA sacn at hip and lumbar spine at entry and annually thereafter • Slit lamp exam at entry and annually thereafter
Study Design • Pt. were seen every 12 weeks to confirm vital status, record any unscheduled visits to health care providers , and note the occurrence of any adverse events. • Post bronchodilator spirometry performed and health status assessed every 24 weeks. • An independent safety and efficacy data monitoring committee performed safety reviews every 6 months. • In addition , 2 interim efficacy analyses were performed , the first after first 358 deaths and the second after a total of 680 deaths.
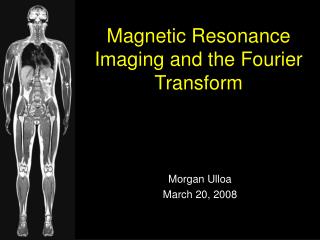
Enrollment of Patients (Figure 1) 8554 Patients recruited 2370 (27.3%) Patients withdrew during run-in period 266 Adverse event unrelated to the study 355 Consent withdrawn 33 incomplete data 5 Lack of efficacy of a nonstudy drug 1638 Entry criteria not met 73 Other reasons 6184 underwent randomization 1546 combination therapy group 1546 safety population 1551 Fluticasone group 1552 safety population 1545 placebo group 1544 safety population 1542 salmeterol group 1542 safety population 13 (0.8%) Excluded 17 (1.1%) Excluded 21 (1.4%) Excluded 21 (1.4%) Excluded 1533 received salmeterol plus fluticasone proponate 50ug/ 500ug twice daily 1534 received fluticasone proponate 500ug twice daily 1521 received salmeterol 50ug twice daily 1524 received placebo
Enrollment of Patients (Figure 1) 1533 received salmeterol plus fluticasone proponate 50ug/ 500ug twice daily 1521 received salmeterol 50ug twice daily 1535 received fluticasone proponate 500ug twice daily 1524 received placebo 673 (44.2%) With drew 366 Adverse event 136 consent withdrawn 21 Loss too followup 103 Lack of efficacy 4 Entry criteria not met 19 Non compliance with regimen 24 Other reasons 587 (38.3%) With drew 360 Adverse event 118 consent withdrawn 24 Loss too followup 45 Lack of efficacy 4 Entry criteria not met 16 Non compliance with regimen 20 Other reasons 522 (34.1%) With drew 289 Adverse event 119 consent withdrawn 29 Loss too followup 33 Lack of efficacy 3 Entry criteria not met 20 Non compliance with regimen 29 Other reasons 561 (36.9%) With drew 303 Adverse event 133 consent withdrawn 15 Loss too followup 63 Lack of efficacy 2 Entry criteria not met 19 Non compliance with regimen 26 Other reasons 851 completed the study 960 completed the study 947 completed the study 1011 completed the study
Agenda • COPD Introduction • Journal Introduction • Background & Hypothesis • Study Design • Study Population • Demographics • Mortality Analysis • Efficacy Analysis • Summary
Study Population • Inclusion Criteria • Current and former smokers with 10 pack-year history of smoking. • Male & Female, age 40-80 yr. • Pre bronchodilator FEV1 less than 60 % predicted. • FEV1 increase of less than 10% with use of 400 microgram of Albuterol. • Ratio of pre-bronchodilator FEV1/FVC less than or equal to 0.70. • An established history of COPD
Study Population • Exclusion Criteria • Current diagnosis of Asthma or Resp. disorder other than COPD • Chest radiograph indicating diagnosis other than COPD • Lung volume reduction surgery and/or lung transplant • Requirement for LTOT at start of study > 12h.day • Receiving long-term oral corticosteroid therapy • Serious, uncontrolled disease likely to interfere with study and/or cause death with in the 3yr study period
Study Population • Mean Age = 65 yrs • Mean post-bronchodilator FEV1=44% of predicted value • One yr before entry in to study, more than half the patients had used inhaled corticosteroids, LABA or both • 57% of patients had reported an exacerbation • Compliance to treatment was similar in all groups ranging from 88%-89% of the prescribed dose taken
Agenda • COPD Introduction • Journal Introduction • Background & Hypothesis • Study Design • Study Population • Demographics • Mortality Analysis • Efficacy Analysis • Summary
Proportion of patient who withdrew from study was : • Highest in placebo group (44%) and • Lowest in combination therapy group (34%)
Agenda • COPD Introduction • Journal Introduction • Background & Hypothesis • Study Design • Study Population • Demographics • Mortality Analysis • Efficacy Analysis • Summary
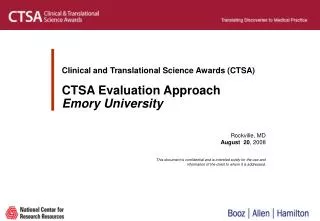
Mortality Analysis • At 3 yrs vital status was known for 6111 of the 6112 patients included in efficacy population • There were 875 deaths in 3 yrs • Absolute risk reduction for death in combination therapy group vs. placebo was 2.6% • Hazard ratio was 0.825 and reduction in risk of death was 17.5% • Risk of death in combination therapy group … • did not differ significantly from salmeterol group. • was less than fluticasone group. • Risk of death from all causes was similar to risk of death from COPD (data not shown)
Combination therapy group reduced the risk of death by 17.5% at any time during 3 years
6.0% • 6.1% • 6.9% • 4.7%
Agenda • COPD Introduction • Journal Introduction • Background & Hypothesis • Study Design • Study Population • Demographics • Mortality Analysis • Efficacy Analysis • Summary
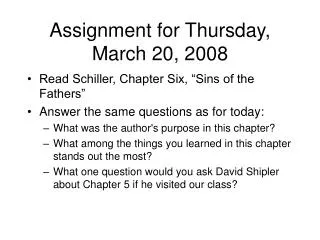
Efficacy Analysis • Exacerbations • 25% reduction in combination therapy group compared to placebo • NNT = 4 to prevent one exacerbation in 1 yr • 26% patients were hospitalized during 3 years study period • Annual admission rates were 17% lower in combination therapy and salmeterol group than in placebo group. • NNT = 32 to prevent one hospitalization