Download
1 / 35
350 likes | 476 Views
Does where you live influence your health or the reporting of ill-health?. Michael Rosato, Gemma Catney, Sheelah Connolly, Seeromanie Harding, Dermot O’Reilly. Std Mortality Rates. Self-reported Health. Std Mortality Rates.

E N D
Does where you live influence your health or the reporting of ill-health? Michael Rosato, Gemma Catney, Sheelah Connolly, Seeromanie Harding, Dermot O’Reilly
Self-reported Health Std Mortality Rates
Project 019: Variations in alcohol related deaths in Northern Ireland Background: • Globally 4% of all deaths • Impact on crime, productivity and families • Costs ~£20billion/year in England • Epidemiology not entirely clear • Ecological studies show strong association to area deprivation and urban living
Aims • To examine differences in alcohol-related mortality between areas • Urban/rural • Affluent/deprived • To determine if these differences were due to characteristics of the individuals living in these areas or to specific area effects.
Data (i) • Northern Ireland Mortality Study (NIMS) • 720,627 people aged 25-74 • Non-institutionalised • Age, sex, marital status, • LLTI & GH • SES, NS-SEC, Educ attainment, • Housing tenure & cars (for area deprivation only) • Area: • Income domain of NIIMD • Settlement band (Urban, intermediate, Rural)
Data (ii) ICD-10 codes for alcohol-related deaths: F10—mental and behavioural disorders due to use of alcohol; G31.2 - degeneration of nervous system due to alcohol; G62.1- alcoholic polyneuropathy; I42.6- alcoholic cardiomyopathy; K29.2- alcoholic gastritis; K70- alcoholic liver disease; K73- chronic hepatitis, not elsewhere classified; K74- fibrosis and cirrhosis of liver (excluding K74.3-K74.5—biliary cirrhosis); K86.0- alcohol-induced chronic pancreatitis; X45- accidental poisoning by and exposure to alcohol; X65- intentional self-poisoning by and exposure to alcohol; and Y15- poisoning by and exposure to alcohol, undetermined intent. Deaths: 5-years follow-up 578 alcohol related deaths
Conclusions: • Higher mortality risk for disadvantaged individuals. • No independent effect of area deprivation. • Mortality lower in rural areas. Explanations for these findings?? Area of residence and alcohol-related mortality risk: A five–year follow-up study. Connolly S, O’ Reilly D, Rosato M, Cardwell C. (Addiction DOI: 10.1111/j.1360-0443.2010.03103.x)
Project 011: Area influences on health: does community or religious segregation matter?
Background/theory • Good • Bad Aims: • Variations in mortality risk across different levels of denominational concentration • Variations in cause-specific mortality
Mortality risk by level of concordance Model 1 is adjusted for age(in 5-year bands), sex and marital status; Model 2 is Model 1 further adjusted for educational activity, NS-SEC, housing tenure, car availability, economic activity, house value and settlement band
Conclusions • The more polarized areas are the most deprived • Mortality is higher in the more polarized areas • The higher mortality in concordant areas is due to SES. • The higher mortality of Catholics in Protestant areas (and to a lesser extent, of Protestants in the most Catholic areas) is unexplained. • Clues in cause-specific mortality? • Overall living in discordant areas may be bad for health??? • Other explanations are possible
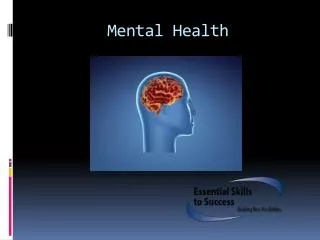
Project 015: The socio-economic (& cultural influences) on the perception & reporting of self-reported health in NI Does a weak labour market make people feel sick? Dissonances in self-reported health and mortality across denominational groups in Northern Ireland O’ Reilly D, Rosato M. Soc Sci Med 2010; 71: 1011-1017
Self-reported Health Std Mortality Rates
What happens when people become unemployed? U/E benefits Work No work Health-related benefits
Hypotheses • Where labour market is poor people are more likely to report ill-health • The relationship between SRH and mortality should vary according to strength of labour market Aims: • Logistic regression to explore relationship between labour market and levels of ill-health • Cox proportional hazards to investigate effect modification by areas on SRH-mortality relationship
Data & methods • NIMS with ‘usual suspects’ • Labour market • %working age who are U/E or permanently sick • <10%; 10%-14.9%; 15%-19.9%; 20%-24.9%; 25% and over • Good correlation with %employment; and employment domain of NIIMD • Mortality: 6.7 years of follow-up
Likelihood of reporting a limiting long term illness. Data represent odds ratios (95% confidence intervals) from logistic regression models. ** Adjusted for age, sex, marital status, educational attainment, housing tenure and car availability
Conclusions • Some indication that weak labour market shifts perception of health • Likelihood of reporting poor health is higher where labour market is weakest • Relationship of LLTI to mortality is modified by labour market • Does this have repercussions for the health services?
Thank you Questions?
Acknowledgements The help provided by the staff of the Northern Ireland Longitudinal Study (NILS) and NILS Research Support Unit (RSU) is acknowledged. NILS is funded by the HSC R&D function of the Public Health Agency. They also funded some of the projects which comprise this talk. The NILS-RSU is funded by the ESRC and the Northern Ireland government. The authors alone are responsible for the interpretation of the data.