Download
1 / 37
370 likes | 498 Views
HIVI. HIV Initiative of Kaiser Permanente and Care Management Institute. Teaching Physicians to Talk about Sex, Drugs, and Maybe Rock ’n Roll. Or… Can We Do for Prevention What We Have Done for Treatment?. Enid K Eck, RN, MPH Michael Allerton, MS.

E N D
HIVI HIV Initiative of Kaiser Permanente and Care Management Institute Teaching Physicians to Talk about Sex, Drugs, and Maybe Rock ’n Roll. Or… Can We Do for Prevention What We Have Done for Treatment? Enid K Eck, RN, MPH Michael Allerton, MS
Background and History • Lets Review
Treatment Quality Measures • Time to Care: > 90% within 90 days • Maximal Viral Control: > 91% • Consistency of Care: 84%-91% HIV RNA “viral load” & CD4 on time • Co-Morbidity Testing: 94% tested for HCV • Prenatal HIV Screening: 81%->95% • Early Detection: 25.8% CD4 <200 upon Diagnosis • Mortality Rate: <1.0-1.6%/year (3.4% outside KP) These are KP program-wide statistics.
Treatment Quality Measures • BUT MOST IMPORTANT: • These Result Do Not Differ By Race, Gender, or Ethnicity • Within Kaiser Permanente • Across All Regions
What If… We could do the same for Prevention?
BUT… • What do we really know about prevention?
Prevention Is… • HARD!!!! • Invisible when successful • Catastrophic when fails • Not an absolute • Variable over time.
Prevention Is… A CONTINUUM Success Failure
Prevention Is… A CONTINUUM Success Failure Vaccination Smallpox, polio…
Prevention Is… A CONTINUUM Success Failure Cure TB, Syphilis Vaccination Smallpox, polio…
Prevention Is… A CONTINUUM Success Failure Cure TB, Syphilis Vaccination Smallpox, polio… PrEP Malaria… PEP Bacterial Meningitis
Prevention Is… A CONTINUUM Success Failure Cure TB, Syphilis Vaccination Smallpox, polio… Environmental Water Treatment, Closed Sewers, Mosquito abatement… PrEP Malaria… PEP Bacterial Meningitis
Prevention Is… A CONTINUUM Success Failure Behavioral Hand Washing, Abstinence, Condoms Cure TB, Syphilis Vaccination Smallpox, polio… Environmental Water Treatment, Closed Sewers, Mosquito abatement… PrEP Malaria… PEP Bacterial Meningitis
Prevention Is… A CONTINUUM Success Failure AND A CORRELATION Passive Active
Prevention Is… A CONTINUUM Success Failure AND A CORRELATION Passive Active AND FINALLY Harm Elimination Harm Reduction
What’s New? • TLC+ • National Prevention Guidelines
Three Steps to Success • Requirement One: Start Talking • Requirement Two: Talk Some More • Requirement Three: Start Talking to Your Colleagues
Start Talking • The Need: These are US national statistics.
Start Talking • But do you know WHO to talk to?
Women as a Share of New AIDS Diagnoses 27% 27% 20% 13% 8% 1985 1990 1995 2000 2004 Note: Data are estimates. Sources: CDC, Data Request, 2006.
Reported HIV Cases Among Teen Girls and Younger Women, 2003 Females Males 50% 63% 71% 50% 37% 29% 13-19 20-24 25 and older Notes: Data based on person’s age at diagnosis, from 41 areas with confidential name-based HIV surveillance for adults and adolescents in 2003. Source: CDC, HIV/AIDS Surveillance in Adolescents, L265 Slide Series Through 2003.
HIV Spread Primarily Through Sex, Increasingly Heterosexual 3% Heterosexual 13% Other 31% Heterosexual 42% MSM 19% IDU 65% MSM 6% Other 22% IDU 1985 2004 Notes: Data are estimates. May not total 100% due to rounding. Sources: CDC, Presentation by Dr. Harold Jaffe, “HIV/AIDS in America Today”, National HIV Prevention Conference, 2003; CDC, HIV/AIDS Surveillance Report, Vol. 16, 2005.
Proportion of AIDS Cases, by Race/Ethnicity, 1985-2004 70 60 African American 50 40 Percent of AIDS Diagnoses White, non-Hispanic 30 Latino 20 Asian/Pacific Islander 10 American Indian/Alaska Native 0 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2004 Note: Data are estimates. Source: CDC, Data Request, 2006.
Start Talking • But to WHO?
Start Talking • But to WHO?
Start Talking • It is strongly recommended that clinicians routinely obtain a thorough sexual and substance use history from all patients > 12 years of age to assess risk behaviors and stratify for appropriate testing.
Start Talking • Anyone who acknowledges having had unprotected sexual activity • Patients with multiple sexual partners (serial monogamy counts…) • Patients with current or previous STI • Patients with sexual partners with current or previous STI • Patients with history of recreational or intravenous drug use (IDU), particularly methamphetamines • Patients with chronic alcohol abuse • Patients with hepatitis B or hepatitis C • Men who have exchanged money or drugs for sex, who have been incarcerated, or who have had sex with other men. • Women who have exchanged money or drugs for sex.
Start Talking • But What Do I SAY?
Start Talking • ASK… • (It’s not so much what you are saying as much as what you are listening too…)
Start Talking • For All Patients: • “I’d like to ask you some questions related to your sexual health that I ask all my patients.” • Are you sexually active? If no, have you ever had sex? • How many lifetime sexual partners have you had? Timeframe? • Are/were your sexual partners men, women, or both? • Did/do you have vaginal, anal, and/or oral sex? • Have you ever been diagnosed with an STD or thought you might have one? • Has your partner? • Have you ever been tested for HIV or advised to be tested? • Has your partner? • How do you protect yourself from STIs and HIV?
Start Talking • For Married Members and Couples • “I’d like to ask you a few questions related to your sexual health. These are questions that I ask all my patients regardless of the type of relationship they are in.” • Do you or your partner have sex with other people outside of your marriage? • How do you protect yourself from STDs and HIV? • Have you or your partner ever been diagnosed with an STD? • Have you or your partner ever been tested for HIV? • How long have you been married/together? • Before you were a couple did you have sex with other people? • If yes, with men, women, or both? • Before you were married, did your partner have sex with other people? • If yes, with men, women, or both?
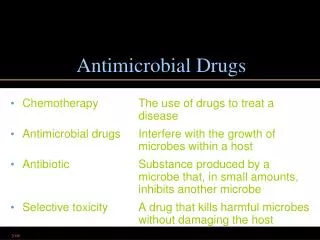
Talk Some More • Screen: • It is strongly recommended that patients be appropriately screened for HIV infection and STI based on their individual risk assessment.
Talk Some More • Screen: • Screen and promptly treat all identified individuals > 12 years of age at risk sexually active adults and adolescents for the following STIs – • Human immunodeficiency virus (HIV) • Neisseria gonorrhea • Chlamydia trachomatis\ • Syphilis • Hepatitis B • Hepatitis C • Trichomoniasis (for women) NOTE: Evidence suggests the presence of other STIs, including herpes simplex, increases the risk of HIV transmission and acquisition.[1] [1] From USPSTF-- ‘Based on a paucity of supporting evidence, herpes simplex virus (HSV) serology testing is not routinely recommended.’
Talk Some More • Intervene: • Patients engaging in high risk activities but recently tested negative for HIV are the most important population to target for evidence based prevention strategies and will yield the greatest impact on HIV transmission rates. Care must be taken to keep the negative test from reinforcing the risk behaviors, or being cited as “proof” by the patient that they are not at risk.(36) Untreated depression has been associated with high risk behavior in gay men(37, 38), and persistent substance use contributes to transmission both as a dis-inhibitor to safer practices and as a direct transmission route in inject drug use.
Talk Some More • Intervene:
Talk Some More • Intervene: • Ways to assist the patient in creating a personalized plan for HIV risk reduction: • Avoid language that may be insensitive to patient’s background and which may impair further disclosure • Motivate patients for behavioral change • Offer latex condoms and information on appropriate handling and lubricants to all sexually active persons • Counsel regarding drug use, including alcohol, methamphetamine, and injection drug use • Remind that Oral contraceptives do not prevent HIV or an STI. • Advise to seek prompt treatment for any suspected STI or known exposure to an STI even in the absence of symptoms. • Reassess sexual practices at future visits and plan for repeat testing as appropriate • Avoid false reassurance
Start Talking to Your Colleagues • Roll Out The National Guideline: Your Role