Download

1 / 38
380 likes | 717 Views
Approach to the Patient with Suspected Kidney Stones. Bradley Thomas Oliver The University of South Carolina 12/14/05. Overview. Renal calculi occur in 5-12% of the American population bilateral in 10-15% of patients. 80% of patients with urolithiasis form calcium stones

E N D
Approach to the Patient with Suspected Kidney Stones Bradley Thomas Oliver The University of South Carolina 12/14/05
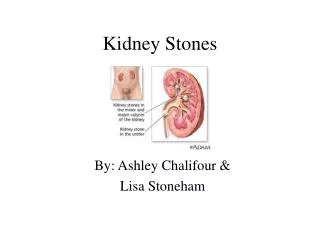
Overview • Renal calculi occur in 5-12% of the American population • bilateral in 10-15% of patients. • 80% of patients with urolithiasis form calcium stones • Most are composed of calcium oxalate • Less often calcium phosphate • The other main types include: • uric acid • struvite (magnesium ammonium phosphate) • cystine stones
Overview Cont • The same patient may have a mixed stone • Another type limited to HIV patients • Indinavir-induced stones • The drug crystalizes and the stones are composed almost completely of the protease inhibitor. • Happens in 4% to 22% of patients treated with the standard dose of indinavir (800mg three times a day) • Stones can cause renal scarring, damage, or even renal failure if they are bilateral. • In 10% of patients, stones recur within 1 year. This percentage increases to 50% within 10 years.
Calcium Stones • In general, calcium phosphate stones are associated with the same risk factors as calcium oxalate stones • Excepttions: Calcium phosphate stones more typical of Type I RTA and primary hyperparathyroidism
Uric Acid Stones • Occur primarily in patients in whom a persistently acid urine (pH<5.5) promotes uric acid precipitation • Example: gout patients that are uric acid overproducers (10-20%) • Also in states of chronic diarrhea
Struvite Stones • Chronic urinary tract infection due to a urease producing organisms such as Proteus or Klebsiella • Often have multiple magnesium ammonium phosphate crystals in the urine sediment • If not adequately treated can develop into a staghorn or branched calculus involving the entire renal collecting system
Cystine Stones • Develop in patients with cystinuria due to the insolubility of cystine in the urine
Diagnosis • Initially suspected by the clinical presentation • Should be suspected in all patients with the acute onset of atraumatic flank pain • Particularly if no abdominal tenderness and with hematuria • Classically: severe colicky flank pain • Often with radiation to the groin, testicles, back, and periumbilical region. • Gross or microscopic hematuria occurs in the majority of patients with symptomatic nephrolithiasis • Other than actually passing a stone or gravel, single most discriminating predictor of a stone in patients with AUFP
Symptoms Cont. • Hematuria, however, is not detected in approximately 10 to 30% of patients with documented stones • Other symptoms: nausea, vomiting, dysuria, and urgency
Passage • Stones smaller than 4 mm pass spontaneously in approximately 80% of patients. • Stones that are 4-6 mm pass in approximately 50% of patients • Stones larger than 8 mm pass in only approximately 20% of patients.
Differential Diagnosis • 1). Bleeding within the kidney • 2). Ectopic Pregnancy • 3). Aortic Aneruysm • 4). Acute Intestinal Obstruction • 5). Malingering
Abdominal Plain Film • Will identify radiopaque stones • Struvite stones • Calcium stones • Cystine stones • Will miss radiolucent uric acid stones • May not detect small stones or stones overlying bony structures • Will not detect obstruction
Abdominal Plain Film Cont. • Reasonable initial test in patients with history of radiopaque calculi and acute pain that is similar to previous episodes • May, however, also miss stones in the ureter
Intravenous Pyelogram • Higher sensitivity and specificity than a abdominal film alone • Provides information about the degree of obstruction • Can produce contrast reactions • Therefore, has been replaced by non-contract –enhanced helical CT as the test of choice
IVP showing right kidney completely obstructed by a 7 mm radiopaque calcium oxalate stone in the proximal ureter • The right kidney appears dense due to accumulated radiocontrast that cannot be excreted. • The left kidney shows a normal excretory phase of the study with contrast in the renal pelvis and ureter.
Non-contrast Helical CT Scan • Gold Standard • Can detect both the stone and urinary tract obstruction • Can also define an alternate significant diagnosis • In one report of patients with their first episode of a suspected kidney stone, 33% had an alternate diagnosis, not suspected on clinical grounds (50% of these had significant disease)
Non-contrast Helical CT compared to IVP • Higher sensitivity and specificity • regardless of its size, location, and chemical composition • Faster • 26 versus 69 minutes • Only slightly more expensive • $600 versus $400 ** Chen, MY, Zagoria, RJ. Can noncontrast helical computed tomography replace intravenous urography for evaluation of patients with acute urinary tract colic?. J Emerg Med 1999; 17:299.
Numbers • Standard CT cuts are generally 8mm, but 3 to 5mm cuts are optimal for the detection of stones • Specificity is nearly 100% • Negative study should prompt consideration of a differential diagnosis
An Exception • Nephrolithiasis secondary to HIV protease inhibitors, primarily indinavir • These stones are not radiopaque and signs of obstruction may be minimal or absent • Contrast-enhanced CT may be needed for diagnosis
Possible Pitfall • In patients who do not have evidence of urinary tract obstruction, the occasional inability to distinguish ureteral stones from phleboliths overlying the course of the ureter
Phleboliths are focal calcified venous thrombi • Frequently seen along the normal anatomical course of the lower ureter. • They are usually the result of injury to the vein wall commonly from venous hypertension and are composed of concentric calcified strata around a central kernel. • Typically, phleboliths are rounded with a central lucency and are seen in the true pelvis often below the distal ureter.
Circumferential periureteral edema, or the soft tissue "rim" sign, described as a rim of soft tissue attenuation seen around the circumference of an intraureteral calculus on non-contract CT • Theoretically, phleboliths will not show a "rim" sign. • Since larger stones result in stretching of the ureteral wall, the "rim" sign tends to be more commonly associated with the presence of smaller stones. • The "comet" sign refers to the adjacent eccentric, tapering soft-tissue mass corresponding to the non-calcified portion of pelvic vein contiguous to a phlebolith.
Ultrasonography • Procedure of choice for patients who should avoid radiation, i.e. those pregnant • Very sensitive for the diagnosis of obstruction and can detect radiolucent stones missed on KUB • May miss small stones and ureteral stones
References • eMedicine. 2005 • UpToDate. 2005 • Urolithiasisby David S Goldfarb, MD and Fredric L Coe, MD, Best Practice of Medicine. October 2003.