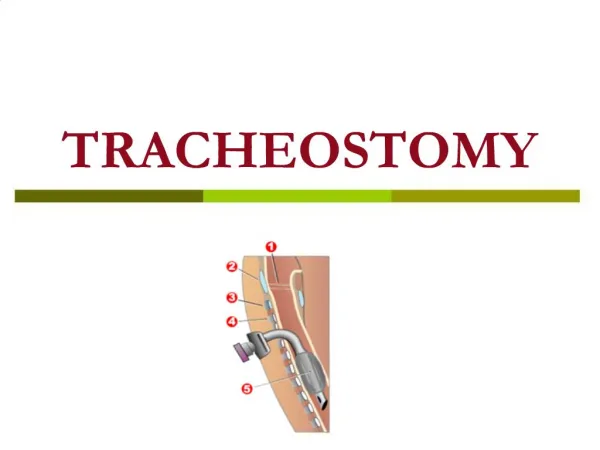
Tracheostomy
Tracheostomy. Dr. Vishal Sharma. Jackson’s metallic tube. Jackson’s metallic tube. Jackson’s metallic tube. Made of German silver (alloy of Ag + Cu + P) Has obturator (pilot), inner tube & outer tube

Tracheostomy
E N D
Presentation Transcript
Tracheostomy Dr. Vishal Sharma
Jackson’s metallic tube • Made of German silver (alloy of Ag + Cu + P) • Has obturator (pilot), inner tube & outer tube • Inner tube is longer than outer tube for its removal & cleaning. Outer tube maintains patency. Pilot is inserted into outer tube for smooth & non-traumatic insertion of tube • Lock prevents expulsion of tube during cough
Fuller’s metallic tube • Outer tube bi-valved. The 2 blades when pressed together, help in smooth entry of tube. • Inner tube is longer & has a vent for phonation • Pt phonates by closing main tube opening • Vent also helps in decannulation of tube
Portex cuffed tube • Made of siliconized PolyVinylChloride. It is thermolabile & prevents crusting. • Low pressure high volume cuff maintains an air-tight seal required for: • Prevention of aspiration of secretions • Positive pressure ventilation
Portex uncuffed tube For tracheostomy patient receiving radiation
Adjustable flange tube Used in obese neck, oedema neck
Salpekar double cuff tube Prevents ischemic necrosis of tracheal cartilage
Functions of Tracheostomy 1. Relieves upper airway obstruction 2. Improves alveolar ventilation by ing dead space by 30-50% & ing airflow resistance 3. Prevention of aspiration of blood & secretions 4. Removal of airway secretions in patient with inability to cough or with painful cough 5. Administration of anesthesia
A. Respiratory obstruction Trauma to airway : external, endoscopic Infection: epiglottitis, croup, Ludwig’s angina, para-pharyngeal /retro-pharyngeal abscess Neoplasm: laryngo-tracheal, pharyngeal Foreign bodyin airway Oedema of larynx: irritant, allergic, irradiation Paralysis of larynx: B/L abductor palsy Congenital: laryngeal web, cyst, choanal atresia
B. Retained airway secretions Inability to cough: coma, respiratory muscle palsy or spasm, laryngectomy Painful cough: chest injuries, pneumonia Excessive secretions: pulmonary oedema C. Respiratory insufficiency Chronic bronchitis, bronchiectasis, atelectasis, reatined airway secretions
D. Anesthesia administration in: Laryngo-pharyngeal growths Maxillo-facial trauma Trismus Severe Ludwig’s angina Positive pressure ventilation for > 72 hrs
Types of Tracheostomy Emergency Elective Temporary Permanent Therapeutic Prophylactic • High (1st ring): above thyroid isthmus • Mid (2nd – 4th ring): behind thyroid isthmus • Low (below 4th ring): below thyroid isthmus
Mid tracheostomy preferred High tracheostomy leads to subglottic stenosis Low tracheostomy is avoided as: Trachea is deeper Displacement of tracheostomy tube is common Proximity to great vessels Surgical emphysema is common Tracheostoma is close to tracheal bifurcation
Positioning Supine position with extension of neck. General anesthesia with endotracheal intubation.
Infiltration Cricoid palpated & a 5 cm horizontal incision marked 2 cm below it 2 % lignocaine & 1 in 2 lakh adrenaline injected into incision line
Horizontal Incision A 5 cm horizontal incision made with # 15 blade & deepened below subcutaneous tissue
Vertical Incision A 5 cm midline vertical incision can be made below cricoid in emergency tracheostomy. This avoids injury to blood vessels.
Exposure of strap muscles Investing layer of deep cervical fascia opened vertically with artery forceps. Palpation for tracheal rings done regularly during the dissection.
Exposure of thyroid isthmus Strap muscles retracted laterally with Langenbeck retractors to expose the trachea & thyroid isthmus
Isthmus separation from trachea Thyroid isthmus detached from tracheal surface & retracted with blunt tracheal hook.
Division of thyroid isthmus If required, thyroid isthmus is divided between clamps. Transfixion sutures applied at the ends.
Confirmation of trachea • 5 ml syringe containing 4 % Lignocaine taken, its needle inserted into trachea & aspirated. Air bubbles confirm presence of needle in trachea. • 2 ml of solution injected into trachea & needle removed quickly to avoid breaking of needle during violent cough movements.
Creation of tracheal window Sharp cricoid hook inserted below cricoid to steady trachea. Tracheal window created by excising anterior 1/3rd of 2nd & 3rd tracheal ring with No. 11 blade & Allis tissue forceps.